Medicare price negotiations were long the pharmaceutical industry’s bête noire, making the 2022 Inflation Reduction Act, which allowed them to proceed on a small number of drugs, one of the sector’s greatest legislative defeats.
But in 2025, Medicare price negotiations have somewhat taken a back seat to a newer threat — President Donald Trump’s attempt to install a “most-favored nation” pricing policy, whereby drugmakers would be required to lower prices in the U.S. to match those paid in certain other industrialized nations.
Such a policy could be particularly damaging to drugmakers, although the details may limit its actual impact. So far, the industry appears to be exploring ways to meet Trump’s demand in spirit, even if not to as great degree as the president’s announcements have sought. An important signal came in mid-August from Eli Lilly, which revealed plans to raise prices for its diabetes drug Mounjaro in the U.K. and, potentially, some other European countries.
“This rebalancing may be difficult, but it means the prices for medicines paid by governments and health systems need to increase in other developed markets like Europe in order to make them lower in the US,” Lilly said.
Other structural changes could be gathering momentum, too. Reforming pharmacy benefit managers, and the opaque rebate schemes they manage, remains on the political radar, as do changes to the “340B” program for discounting drugs to certain hospitals.
Trump redoubles threats in attempt to strongarm drugmakers on prices
The White House set a 60-day deadline for drugmakers to agree on “most favored nation” prices for Medicaid as well as for newly launched drugs.
By: Jonathan Gardner• Published July 31, 2025
President Donald Trump has threatened 17 large drugmakers with “every tool in [the federal government’s] arsenal” if they don’t take steps to lower the prices of their products in line with those charged in other industrialized nations.
Letters sent to the companies followed up an executive order Trump issued May 12 that seeks to impose a “most favored nation” regime on drug pricing in the U.S. That order was intended to trigger negotiations between the federal government and drugmakers on equalizing prices, but the July 31 letter suggest the sides are still far apart.
The letters were sent to AbbVie, Pfizer, Roche’s Genentech unit and Novo Nordisk, among others, and were posted to his Truth Social account.
In the letters, Trump said he is giving drugmakers 60 days to provide the best international price on all of their drugs to people enrolled Medicaid. He also demanded they provide the best international price for all newly launched drugs; launch direct-to-consumer channels offering drugs at the most favored nation price; and repatriate to the U.S. all increased revenues achieved from higher prices negotiated in foreign countries.
The “letters indicate that industry proposals have fallen short, and from this point forward, President Trump will only accept from drug manufacturers a commitment that provides American families immediate relief from vastly inflated drug prices and an end to the freeriding by European and other developed nations on American innovations,” a White House fact sheet stated.
In comments during earnings calls in July, pharma executives said that, in talks with the White House, they have brought up how pharmacy benefit managers’ rebating practices driving up U.S. costs as well as other countries’ negotiating power in lowering their prices.
“The U.S. can no longer pay for the R&D for the world,” said AstraZeneca CEO Pascal Soriot in a company call in July. “We did make our proposals, which we believe could achieve what the President is trying to achieve, but we also need Europe to increase their share of GDP allocated to innovative pharmaceuticals.”
That was echoed by the industry group PhRMA. “Importing foreign price controls would undermine American leadership, hurting patients and workers,” Alex Schriver, the group’s senior vice president, said in a statement.
Wall Street analysts were divided on the announcement’s impact. Leerink Partners’ David Risinger called the proposal “unachievable,” impairing drugmakers’ ability to develop innovative drugs and compete with China-based rivals.
Evercore ISI’s Umer Raffat, on the other hand, said the letters pointed to an improvement in the most-favored-nation plan because Trump’s threat was limited to Medicaid, rather than the much larger Medicare program for older people. He added that applying most-favored nation prices to new drugs will give pharma companies leverage to gain higher prices overseas because they could point to U.S. policy for their refusal to negotiate a lower price.
Article top image credit: Getty Images
Lilly sends a drug price signal in response to Trump threats
As the Trump administration works to implement a “most-favored nation” policy, Lilly said it’s “rebalancing” drug prices to “align” costs across different countries.
By: Jonathan Gardner• Published Aug. 14, 2025
Eli Lilly in August responded to a Trump administration plan to lower U.S. drug costs by issuing a statement claiming it will raise prices in European countries to “align” them with the costs paid “across developed countries.”
The Aug. 14 statement, which wasn’t attributed to any specific Lilly executive, said the effort includes an agreement with the U.K. government to hike the price of the company’s blockbuster diabetes medicine Mounjaro “while maintaining access” for people with the disease.
Lilly didn’t commit to cutting U.S. prices. But it did say that for prices to be reduced in the U.S., the amounts “paid by governments and health systems need to increase in other developed markets like Europe." The company is working with other, unspecified governments and expects to make “any necessary pricing adjustments” by Sept. 1.
Lilly didn’t specify how it will raise prices in those countries — many of which have nationalized healthcare systems that negotiate drug costs for their entire population — without affecting access. It also didn’t reveal whether the planned hikes would be tied to a drug’s list price or the confidential rebate deals cut between drugmakers and national customers.
The statement also pointed out the difficulty of lowering prices in the U.S. because of the healthcare system’s structure.
“The U.S. system is complex and opaque, with multiple cross subsidies, abuse of government programs like 340B, and insurance cost-sharing burdens for patients,” Lilly said.
Through an executive order signed in May, President Donald Trump aims to link the price paid for drugs in the U.S. to the lowest price paid in other high-income countries. This “most favored nation” policy is also meant to spur price negotiations between the federal government and companies, as well as to push drugmakers to establish new ways to distribute medicines to patients at a reduced cost.
Letters the administration sent to executives at 17 drug companies in July redoubled that effort while vaguely warning of consequences for companies that don’t comply.
The “most favored nation” policy has come alongside the threat of tariffs on pharmaceuticals, which has spurred many large drugmakers — Lilly among them — to promise to invest billions of dollars in U.S. drug manufacturing.
In its statement, Lilly reiterated its objections to pharmaceutical levies, arguing they’d “raise costs, limit patient access, and undermine American leadership, especially for companies already investing heavily in domestic manufacturing.”
“We urge the administration and Congress to prioritize strategic incentives that strengthen U.S. manufacturing and supply‑chain resilience without sacrificing access, affordability, innovation, or American leadership,” Lilly said.
Article top image credit: Scott Olson via Getty Images
Sponsored
Inflation reduction act and maximum fair price: Possible industry and practice impacts
By: Nancy McGee, JD, MPH, DrPH, Senior Vice President, Health Policy and Public Payers, Lumanity & Robert Shepherd, MBA, Senior Advisor to Lumanity• Published Aug. 1, 2023
The Inflation Reduction Act (IRA) provides Medicare with the opportunity to negotiate drug prices. While there is preliminary direction about how maximum fair price (MFP) will be calculated, speculation exists regarding how the negotiation process will work, evolve over time, and impact other areas of drug innovation and physician reimbursement. This aspect of the IRA will likely change choices manufacturers make about bringing a new product to market, could potentially dampen investment in additional indications after introduction, and could discourage subsequent class entrants (i.e., follow-on drugs). At the same time, there is the potential for other less obvious unintended market consequences that may change patient access to care, physician reimbursement, and pricing in other payer/purchaser segments beyond Medicare.
The negotiation process for eligible small molecule drugs will start seven years after US Food and Drug Administration (FDA) approval and will go into effect in year nine. For biologics, the process will begin eleven years after licensure and will go into effect in year thirteen. Beyond total product costs in Medicare, other elements that must be considered by the Secretary of Health and Human Services in calculating an MFP include: the cost of producing the drug, research and development costs, any prior federal financial support, and alternative treatments.1
The negotiation of drug pricing and setting of an MFP will alter the revenue curve for manufacturers. With less revenue to fund research and development, budgets could become more selective in funding clinical studies for new products. A primary consequence of this change will elevate the importance of bringing drugs to market with clear revenue pathways. While many respected thought leaders have already expressed concern that innovation for small molecules will be disproportionately impacted due to the brevity of the nine-year period before MFP can be established, there are many other equally concerning consequences associated with MFP implementation.
For example, drugs that are disproportionately used in the 65+ years population may have fewer products in the development pipeline in the long run. These products often require significant research and development investment and address an elderly patient population that is often in the most need of innovation. If the exclusivity time period shrinks due to the MFP, it is conceivable that development efforts could shift to those conditions with larger commercial patient populations and longer exclusivity periods. Another potential consequence is that post approval clinical studies may be deprioritized or eliminated due to the dampened patent protection when an MFP is established. There also may be a similar disincentive for the investment in follow-on drugs which today are important clinical options for patients who either are not able to tolerate or experience side effects with the first entrant. These follow-on drugs often provide greater price competition during the early stages of patent exclusivity.
The value of each indication will be an important business consideration for multiple indication products. Some manufacturers may choose to wait until the clinical studies for the largest indication are completed before submitting a regulatory filing and starting the clock for the MFP process. This is contrary to current launch strategies that begin with smaller indications which can be supported by evidence from a proportionally sized clinical trial, and then gradually grow into larger indications as more clinical evidence and real-world experience is gathered. The market may experience fewer products with multiple indications if it is determined that additional indications are unable to be funded.
There is the potential for broader unintended consequences to occur as a result of the implementation of MFP within the Part B benefit, as well as availability of MFP to state Medicaid programs and 340b Covered Entities as specified in the IRA. For example, MFP may gradually change the reimbursement paradigm in physician offices if it results in a decrease of a drug’s Average Sale Price (ASP) which would alter provider reimbursement. Currently there is no clarity on how manufacturer discounting practices would be modified to account for this reimbursement decline.
As has been observed in oncology, community-based physician practices are dependent upon payer reimbursement of physician-administered drugs. If ASP is diminished, practices with high Medicare patient populations which acquire and administer drugs to their patients may not be able to afford to stay in practice. As a consequence, more physicians might choose to join health systems which as proposed in IRA will gain access to the MFP via the 340b program. This could stimulate even greater volumes of drug purchases through 340b than has been observed to date. This may exacerbate a trend noted by Adam Fein whereby 340b pricing coupled with greater reimbursement rates negotiated by local market dominant health systems have increased - not decreased - healthcare costs.2
A final consequence of note may be acceleration of enrollment in Medicare Advantage programs. In contrast to Prescription Drug Plans (PDPs) that may implement more restrictions as their cost share increases, the Medicare Advantage (MA) programs are incented to offer better access to expensive new drugs due to their value in offsetting costs in other areas of the health benefit spend. As a result, more individuals may opt to participate in Medicare Advantage programs to have access to new drug innovations. The ultimate effect could be a larger portion of Medicare patients being subject to restrictive provider networks implemented by MA programs.
As we move toward the first set of ten Medicare Part D drugs entering the negotiation process, it will be important for manufacturers to start evaluating their product portfolios now to ensure their business models support critical choices about indications and timing to market. In addition, physicians will need to monitor any erosion of ASP to determine ways to streamline their practices. For those that are heavily dependent on Medicare reimbursement, they may choose to join health systems with greater ability to take advantage of drug discounts. At the same time, Medicare-eligible individuals will need to evaluate and select plan options that support access to the drug innovations they need. Perhaps the most important consideration throughout IRA implementation is for CMS and industry stakeholders to develop implementation approaches with an eye on minimizing the unintended consequences that could either harm patient access to, or potentially dampen investment in, the research and innovation that has historically brought significant advancements to public health in the US.
Pharma prepared to work with Trump on DTC drug sales: Pfizer CEO
Pfizer’s Albert Bourla told investors that major drugmakers are “ready to roll up their sleeves” and build out more direct-to-consumer options for their products.
By: Ned Pagliarulo• Published Aug. 5, 2025
Pfizer and other large pharmaceutical companies are taking seriously President Donald Trump’s demand that drugmakers make more of their medicines available direct to consumers in the U.S. at lower cost, Pfizer CEO Albert Bourla said Aug. 5.
“We have serious discussions in the industry,” Bourla told investors on a conference call Pfizer held to discuss its earnings for the second quarter. “I’m connected very often individually with all the major companies and they are all ready to roll up their sleeves and execute something like that.”
Pfizer and partner Bristol Myers Squibb recently announced plans to offer their widely-used blood thinner Eliquis at a discounted cash price through an online service. The company previously launched a direct-to-consumer service that allows patients to book telehealth appointments, schedule vaccinations and fill prescriptions for certain medicines, such as those Pfizer sells for migraine and COVID-19.
“We think it is a fantastic way to go ahead, so we will work collaboratively to do it,” Bourla said.
Obesity drugmakers Eli Lilly and Novo Nordisk have also recently opened up more ways for cash-paying patients to access their weight loss medicines directly. Other companies are signaling interest, too, in exploring ways to sidestep pharmacy benefit managers. These drug-purchasing middlemen extract from drugmakers rebates that insurers say they use to lower overall costs, but not necessarily in ways that are obvious to a prescription-filling patient.
Expanding direct-to-consumer options was one of four demands Trump made of the pharmaceutical industry in letters issued in late July to 17 drugmakers, including Pfizer.
In those letters, the president threatened to use “every tool” the U.S. government has available if the companies don’t take steps to lower the cost of their products to the prices paid in other industrialized countries. Such a “most favored nation” policy could be a major blow to the industry, although analysts are divided on how sweeping its impact would be if limited only to Medicaid, as Trump indicated.
On the Aug. 5 call, Bourla said he is in “active discussions” at the “highest levels of the U.S. government,” including conversations with Trump, Health and Human Services Secretary Robert F. Kennedy Jr., and Centers for Medicare and Medicaid Services Administrator Mehmet Oz. In addition to leading Pfizer, Bourla is the current board chair of industry lobbying group PhRMA.
“The letter asks a lot from us,” Bourla added. “But we are engaged in productive discussion with them and in general I’m happy with the way that they listen to us.”
Pricing threats aren’t the only challenge drugmakers face in the U.S. The Commerce Department is nearing the end of an investigation into pharmaceutical imports expected to result in sector-specific tariffs. In early August, Trump told CNBC that his administration will initially impose a small levy on pharmaceuticals that could later rise as high as 250% over time.
Such duties would be costly for drugmakers, but analysts believe a phase-in period would allow many companies to adjust their supply chains in such a way that the worst financial hit could be mitigated. Already, most of the largest drugmakers have announced major manufacturing investments in the U.S.
Pfizer anticipates that it can absorb the impact of tariffs this year, as well as any changes it makes to its products’ prices, while still meeting its financial forecast of $61 billion to $64 billion in revenue.
Article top image credit: Jacob Bell/BioPharma Dive
Ozempic, Ibrance among next drugs picked by Medicare for price talks
Announcement of the 15 medicines chosen for the second round of negotiations was one of the Biden administration’s final health policy acts.
By: Ned Pagliarulo• Published Jan. 17, 2025• Updated Jan. 17, 2025
Semaglutide, the popular drug sold by Novo Nordisk as Ozempic for diabetes and Wegovy for weight loss, is among a group of widely used medicines selected by the U.S. government for the next round of price negotiations under a 2022 law aimed at curtailing pharmaceutical costs within Medicare.
The Biden administration released the list of 15 drugs on Jan. 17 in one of its final acts of healthcare policy before President Donald Trump took office on Jan. 20.
Publication of the list kicked off a monthslong process that will feature a series of meetings between drugmakers and the Centers for Medicare and Medicaid Services, which oversees the Medicare insurance program. The negotiations, which drugmakers have opposed vociferously, will yield “maximum fair prices” that take effect in 2027.
Also on the list are Xtandi, Ibrance, Calquence and Pomalyst, blockbuster drugs for cancers of the prostate, breast, blood and bone marrow. Trelegy Ellipta, an inhaler used for asthma and chronic obstructive sleep apnea, is included, as are Otezla, a psoriasis medicine, and Vraylar, an antipsychotic.
Ozempic and Wegovy are particularly significant inclusions. Their use in the U.S. has skyrocketed due to the potency of semaglutide, which is the active ingredient of both, in helping control diabetes and shed weight.
Currently, Medicare is barred from covering drugs solely for weight loss. Wegovy is also approved to lower cardiovascular risk in people with heart disease who are either overweight of who have obesity, however.
Some 5.25 million people covered by Medicare took one of the 15 selected medicines between November 2023 and October 2024, according to information provided by CMS. Over that period, gross spending by Medicare on those products totaled $41 billion, or about 14% of total prescription drug costs under the program’s “Part D” benefit.
Medicare’s power to negotiate drug prices in this fashion is newly granted by the Inflation Reduction Act, which Congress passed two years ago in a significant defeat for the pharma industry.
For the first time, the law allows Medicare to use its scale and market power to extract price concessions from drug companies on certain, select medicines. Only “single-source” branded drugs that lack generic competition and are among the 50 products with the highest spending in Medicare Part D can be picked. Part B drugs, which include medicines administered by physicians, are exempt from the first two cycles of negotiations.
The Inflation Reduction Act also specifies that selected drugs must have been on the market in the U.S. for either seven or 11 years depending on whether they are small molecules or biologics, respectively.
CMS chose 10 drugs for the first round, which concluded last summer with the publication of the discounted prices government negotiators extracted from companies. According to the agency, the new prices were on average 38% to 79% lower than the drugs’ list price, or wholesale acquisition cost.
Assessing savings from those efforts is complicated, however. Health plan sponsors that contract with the government to administer Part D benefits already secure drugmaker rebates that can result in lower net prices. Those net prices are not public, so it’s hard to precisely compare the negotiated prices on the first 10 drugs, which take effect in 2026, to what Medicare paid previously.
For this second round, CMS tweaked the rules guiding negotiations, allowing for more meetings with drugmakers and greater input from patients and physicians.
The pharma industry has lambasted the process as essentially price-setting, rather than a true negotiation, because the Inflation Reduction Act gives CMS the power to levy exceptionally steep fines if drugmakers don’t accept the offered “maximum fair price.”
During the first round of negotiations, CMS said it revised its initial offers upwards over the course of meeting with drugmakers. For five of the 10 drugs, the agency reached an agreement with the respective drugmaker as a result of a negotiation meeting. For the other five, the relevant company accepted CMS’ final written offer, per a fact sheet published in August 2024.
Drugmakers have also argued the Inflation Reduction Act’s different treatment of small molecules and biologics is skewing R&D incentives away from the former type of medicine, which is often made in convenient oral doses.
A handful of pharma companies have sued to block the law on various grounds, including its constitutionality, but have so far been unsuccessful.
Drugs selected by Medicare for second round of price negotiations
Congress should reconsider breaking up PBMs, experts say
Many proposals to reform the PBM industry miss the forest for the trees, experts said in June. Instead, Congress should go after the oligopoly enjoyed by the “Big Three” PBMs.
By: Rebecca Pifer• Published June 27, 2025
Bipartisan policies in Congress meant to lower drug costs by targeting middlemen in the pharmaceutical supply chain are likely to run up against a fundamental issue: the three major pharmacy benefit managers’ chokehold on the U.S. drug market, experts said during a drug pricing transparency forum held in Washington, D.C. in late June.
Influential lawmakers on both sides of the aisle have gotten behind proposals to force more transparency in the sector, delink PBM compensation from the rebates they negotiate with drugmakers, and ban PBMs from profiting off of the difference between what they charge payers and reimburse pharmacies for a drug.
But the so-called “Big Three” PBMs — CVS’ Caremark, Cigna’s Express Scripts and UnitedHealth’s Optum Rx — currently hold almost complete control over how patients access medications and the cost of those drugs.
Going after their business practices without changing that reality won’t help, experts said June 27 during the Transparency is Rising event hosted by a coalition of small upstart PBMs.
“The solution to this can’t be just to ban existing practices. It has to be to remove the choke points that people have over particular parts of the supply chain,” said Reed Showalter, a former advisor on competition to the White House during the Biden administration and attorney with the Federal Trade Commission.
The PBM ‘pivot’ problem
Caremark, Express Scripts and Optum Rx jointly control 80% of U.S. prescriptions. The companies are all subsidiaries of massive healthcare corporations that also own a major national health insurer and pharmacy business, giving them the ability to influence multiple stages of a drug’s journey from a manufacturer to a patient — and a significant profit motivation to do so, according to experts.
Caremark, Express Scripts and Optum Rx say they use their market power to drive down drug prices for their payer clients and the members they serve.
But that power also allows the Big Three to sidestep past efforts from Washington and the states to affect their business model, Antonio Ciaccia, the president of consultancy 3 Axis Advisors, said.
Ciaccia cited an example from the state of Ohio, which banned spread pricing in its Medicaid program in 2018 after discovering it overpaid PBMs by nearly $225 million in one year due to the practice.
But Ohio didn’t end up saving any money, because the PBMs began paying pharmacies beyond the contractually agreed price and clawing back the difference after the fact, he said.
“What we’re talking about is essentially this: the nimbleness of the industry to pivot around policy reforms,” Ciaccia said.
Instead of targeting specific business practices, Congress and antitrust regulators should instead prioritize weakening the Big Three’s control by reversing years of unchecked integration that have allowed PBMs to find these opportunities for arbitrage, speakers said.
“I’m skeptical when you don’t touch the underlying power of the Big Three PBMs, when they still cover 100 million lives each, when they still have influence over formularies, they’re going to find new avenues to pad their profits,” said Alejandro Molina, a policy advisor for the White House during the Biden administration.
The law, which would force companies like CVS that own both PBMs and pharmacies to divest one or the other, was quickly met with criticism and legal challenges from the PBM industry.
Still, bills with similar provisions were recently introduced in Vermont, Texas and New York, according to the National Community Pharmacists Association.
There’s a window for concrete reform now, given Congress’ attention on the issue and interest from the FTC and the Department of Justice in cracking down on some of the Big Three’s most egregious actions, speakers said.
The FTC, for example, is currently suing Caremark, Express Scripts and Optum Rx for allegedly inflating the cost of insulin, while the DOJ is reportedly investigating UnitedHealth over a variety of antitrust concerns.
“I think there’s a lot of opportunities,” said Charlie Katebi, the deputy director for health at the conservative America First Policy Institute. “There are so many issues where Republicans and Democrats — on many important issues — see things with totally different realities. That is not the case right now.”
Tackling rebates, transparency
Some policies being thrown around in Washington have merit even if they don’t break up the oliogopy enjoyed by the Big Three PBMs, according to the panelists. For example, the Trump administration has signaled interest in reforming rebates that PBMs negotiate with pharmaceutical companies in exchange for including their drugs on plan formularies.
PBMs should voluntarily find ways to move away from the rebate “kickback” system, lest the federal government do it for them, CMS Administrator Dr. Mehmet Oz said in June, also speaking at the Transparency is Rising event.
Going after rebates won’t solve systemic issues with the market for prescription drugs, experts cautioned. The Big Three say they already pass through the vast majority, if not all, of those savings through to their clients.
And reabtes no longer make up the majority of PBM profits, according to research. Instead, manufacturer fees and specialty pharmacy dispensing are making up more and more of PBMs’ bottom lines.
“As long as the Big Three PBMs have the covered lives of their insured parents they are going to find a way to influence formularies, reimbursements, networks in whatever configuration they want,” Molina said. ”I just feel like we are 10 years behind, and that PBMs are already creating new corporate structures, new revenue sources that we’re going to have to regulate in 10 years. So until we tackle the upstream power of insurers and the Big Three PBMs and vertical integration, we’re not really solving any structural issues.”
But transitioning away from a compensation stream directly tied to drug prices may be good in the long run, given the rebating system continues to function in perverse ways, according to Sheehey.
For example, when one corporate parent owns both the PBM and the payer, they do get to retain profit from rebates even if their PBM is ostensibly passing it through.
“This is no disrespect to CVS Health, but when they’re like, ‘Oh, look, Caremark’s not getting a really fat portion of that rebate revenue.’ But then their parent company is? This is a company that has one ticker on all the markets,” Sheehey said.
In the absence of a top-down overhaul, PBM transparency reform to shine more light on contracting practices, pharmacy fees and other financial arrangements is a good starting point to make the market and policymakers more informed, panelists said.
That’s something the CMS is moving toward as well, with Oz saying the agency could issue rules forcing payers to share more information on their drug transactions as soon as this year.
But as Washington appears poised to step into the fray, it’s imperative lawmakers and regulators think about the root problem to avoid creating new ones, according to the panelists. For example, experts said regulatory scrutiny is one reason why major PBMs have spun off affiliated companies like rebate aggregators that live offshore, adding more complexity into the prescription drug supply chain.
“We need to realign incentives more structurally, and in any efforts to change transparency we need to be very careful that we are not basically emboldening the next layer of opacity, because the unfairness hides in the opacity of the system,” said Showalter.
Article top image credit: Win McNamee via Getty Images
Drugmakers score policy win in fight against 340B
A new pilot program from HHS will test alterations to the contentious 340B pricing program by swapping traditional upfront drug discounts for rebates.
By: Amy Baxter• Published Aug. 4, 2025
The Trump administration unveiled new healthcare policies at the end of July, among them a pilot program that will trial a major change that could favor the pharmaceutical industry.
Through the pilot, drugmakers will have an opportunity to test replacing upfront discounts with rebates for certain prescription drugs they provide through the 340B Drug Pricing Program, which provides discounted medications to healthcare centers that serve low-income or uninsured patients.
Several large pharmaceutical companies, as well as the industry’s biggest lobbying group PhRMA, have pushed for a rebate model to replace 340B’s discount structure, which critics argue has been abused by some hospitals. They were recently blocked from doing so proactively, however.
Drugmakers and PhRMA claim a rebate system would improve oversight, reduce duplicate discounts and modernize the program.
Conversely, healthcare industry groups have said a rebate model will harm hospitals by forcing them to cover higher drug prices while they wait to recoup some of their costs.
The Department of Health and Human Services has so far not allowed drugmakers to implement their own rebate models, even after drugmakers sued the agency last year. Under the new pilot, HHS is implementing guardrails by limiting the new approach to just the 10 drugs that were selected for Medicare drug price negotiation in 2026. The model will help the Health Resources & Services Administration, which oversees 340B, understand “the merits and shortcomings of the rebate model,” the administration said.
Rebates vs. discounts
Since the 340B program was established in the 1990s, it has grown to include nearly 60% of all hospitals. This expansion has caught the attention of the pharma industry, which has voiced concerns about abuse in the program and blamed HRSA for not keeping up oversight.
In particular, drugmakers are worried about duplicate discounts, where a hospital allegedly purchases a drug at the discounted rate but also receives a Medicaid rebate. Rebates instead of discounts, they argue, would erase the problem.
“Under a rebate model, a covered entity would pay for the drug at a higher price upfront and then later receive a post-purchase rebate that reflects the difference between the higher initial price and the 340B price,” the HRSA’s announcement on the federal register reads.
That higher upfront cost could translate to millions of dollars that hospitals are forced to temporarily cover. The average annual “float” by hospitals to pharma companies is estimated to be more than $72 million, according to 340B Health, a nonprofit organization representing 340B hospitals and health systems. The financial impact of waiting for rebates could cripple operations for some providers — 27% of hospitals said waiting a month for rebates could hinder payroll and force layoffs, 340B Health found.
Not only will hospitals have to cover more costs — they’ll face new administrative burdens with a rebate model.
“The pilot model's impact on hospitals and health systems introduces several operational, financial and strategic risks,” said Joel Wright, president, pharmacy services at VytlOne, a pharmacy solutions provider. “Managing rebate claims and reconciling payments adds complexity and risk of denied rebates due to technicalities or eligibility disputes.”
Notably, the pilot requires all rebates to be paid within 10 calendar days of submissions, and hospitals will have 45 days from the date of dispensation to submit and report data for rebates.
Because the pilot covers just 10 drugs in the Medicare drug price negotiation program, however, rebate lobbyists say it doesn’t go far enough.
“The administration’s rebate pilot is a positive first step toward addressing hospital abuse of the 340B program, but we believe it should cover all medicines and address broader program integrity concerns,” Alex Shriver, senior vice president at PhRMA, told PharmaVoice in an email.
340B Health disagrees and is concerned about the program expanding further.
“While we recognize the agency’s intent to test a limited rebate model tied to IRA implementation, we remain deeply concerned about the financial and administrative burdens the rebate approach will place on 340B hospitals,” said Maureen Teston, president and CEO of 340B Health. “HRSA says it could choose to expand the list of drugs after next year following its evaluation of the pilot program.”
With HRSA’s announcement, eligible drug manufacturers can apply to participate in the voluntary pilot until Sept. 15, with approvals coming by Oct. 15 and going into effect on Jan. 1, 2026. The Office of Pharmacy Affairs will review and accept pilot applications from drugmakers involved in the Medicare drug price negotiation program for 2026.
A public comment period of 30 days is also open on the federal register.
Pharma’s legal fight
A handful of drugmakers attempted to launch their own rebate models last year, which HRSA blocked. Eli Lilly, Bristol Meyers Squibb, Novartis, Sanofi and Johnson & Johnson sued HHS in an effort to push through their rebate models, but district judges upheld the agency’s authority, declaring HHS has the authority to approve or deny rebate models before they can be effective.
HRSA had several concerns with drugmakers’ rebate models, according to Wright, including a lack of approval, the potential to undermine the program’s safeguards, obscure pricing and eligibility data, as well as complicated enforcement.
While the judges stood with HHS, they did not say such models were prohibited, only that HRSA had to approve them first. The pilot doesn’t suggest outright that drugmakers will be able to implement their own rebate models in the future, but it does give the agency a chance to test a change to the discount structure.
“Limiting the pilot to IRA negotiated drugs represents a strategic trade-off — narrowing the scope from pharmaceutical manufacturers' initial 340B rebate model while enabling the industry to evaluate the model’s effectiveness,” Wright said via email.
Article top image credit: Getty Images
Big pharma’s looming threat: a patent cliff of ‘tectonic magnitude’
Many current top-selling products will lose patent protection by the end of the decade, putting pressure on companies to replace lost revenue with new medicines.
By: Jonathan Gardner• Published Feb. 21, 2023
Editor’s note: This story was published in February 2023 and has been lightly updated to ensure date references are consistent and accurate. We’ve included it here as the story’s main points still hold and continue to shape drugmaker strategy.
At the start of the last decade, big pharma was getting smaller. Blockbuster medicines that had fueled years of growth were losing patent protection, exposing the industry’s largest companies to generic competitors. The resulting impact was so substantial it temporarily stalled the relentless upward march of U.S. drug spending.
Today, big drugmakers are facing an even larger “patent cliff,” with more than $200 billion in annual revenue at risk through 2030. But this time around, many of the brand name drugs losing market exclusivity are biologic products, manufactured from living cells, rather than the chemical pills that previously dominated the ranks of pharma top-sellers.
These biologic drugs, like AbbVie’s anti-inflammatory treatment Humira and Merck & Co.’s top-selling cancer medicine Keytruda, face competition from so-called biosimilar drugs that, unlike generics, may not be as easily substitutable. Still, it will be a treacherous period for drugmakers to navigate, as they will need to replenish their research pipelines and carefully manage new product launches to replace lost revenue.
“This is of tectonic magnitude,” Arda Ural, health sciences markets leader at the consultancy EY. The looming patent expirations "capture most blockbusters," he added.
Besides Humira and Keytruda, drugs like Bristol Myers Squibb’s immunotherapy Opdivo, Johnson & Johnson’s immune disease medicine Stelara and Regeneron’s eye treatment Eylea will reach the end of their patent protection this decade.
The launch of copycat versions to Humira in 2023 represented a start of sorts for this looming industry-wide patent cliff. While their market share remains miniscule, their entry has forced AbbVie to negotiate more aggressively to secure insurance contracts. As a result, U.S. sales of the drug, which totaled $18.6 billion in 2022, fell to $12.2 billion in 2023.
A different sort of cliff
The pattern of sales decline for Humira and other blockbuster biologics like it is expected to be different for several reasons, though.
Many biosimilars won’t be interchangeable, or directly substitutable, by pharmacists, for example. Physicians, meanwhile, may be reluctant to switch patients who are stable on the branded drug, meaning that initially it will be newly diagnosed patients with chronic diseases who are most likely to receive biosimilars. And because biosimilars are more expensive to develop and make, their manufacturers won’t be able to afford cutting prices by nearly as much as with generic pills.
“If you track the sales of a typical small molecule that goes generic it really goes off the cliff — 80% of the market can be gone in 30 to 90 days and the price goes down even more,” said Richard Kelly, a senior partner with the law firm Oblon, McClelland, Maier & Neustadt who specializes in life sciences intellectual property.
“[Biosimilars] have to be sold,” he added. “[Salespeople] have to go around to the doctors to sell a drug. It’s just another product in the detail-man’s bag.”
Take the statin Lipitor, once the world’s most lucrative drug. Sales fell from nearly $11 billion in 2010, the year before it faced generics in the U.S., to $4 billion in 2012. Pfizer’s overall revenue fell from $68 billion to $59 billion over the same period.
A pen and carton of Amgen’s Humira biosimilar Amjevita
Permission granted by Amgen
In the case of Humira, the fall is expected to be more gradual, with the company forecast to retain more than one-third of its 2022 U.S. revenues in 2024 and hold onto more than $2 billion through 2030, according to Evaluate Pharma.
The impact will be felt, nonetheless: AbbVie’s revenue fell in 2023 because of Humira competition. And AbbVie executives have indicated sales are likely to be sluggish in 2024, too, walking back previous predictions the company would see a return to growth then.
Humira’s sales erosion will be closely watched throughout the industry as executives and investors try to understand the long-term effects of biosimilar entry. Early biosimilars didn’t impact prices the way that payers and lawmakers had hoped, in part because there weren’t many of the copycat drugs. (While 46 biosimilars are now approved in the U.S., some are not available on the market.) Branded drugmakers also successfully used contracts and rebates to stave off competition.
However, analysts and industry experts believe the sheer number of Humira copycats and the entry of interchangeable products will allow them to take share from AbbVie.
The chief question facing AbbVie is how quickly it can recover through two replacement products: Skyrizi for psoriasis and Crohn’s disease, and Rinvoq for rheumatoid arthritis and several other inflammatory disorders. The company has upgraded its forecasts for both drugs, which it now says will earn $21 billion combined in 2027, approximately equalling Humira’s peak sales.
One major reason Humira achieved its massive sales was the many different autoimmune disorders for which it gained approval. With follow-on biologic drugs, however, the incentives to do so may be limited by the Inflation Reduction Act, which gives the federal government the power to negotiate lower prices within Medicare, said Mara Goldstein, Mizuho Securites’ senior biopharma analyst.
“We’re living through this real time and it’s a little challenging,” she said. “Does it truly create a disincentive to develop indications? Will companies continue to invest in new clinical trials right up to patent cliffs? How does [the law] change the value of dollars invested over time?”
New lessons to learn
AbbVie followed the lessons of the previous patent cliff by merging with Allergan in a 2019 deal that gave it enough new revenue to withstand the expected erosion of Humira's sales. Its approach was similar to large pharmaceutical companies’ strategy ahead of the 2010s patent cliff, which spurred the megamergers of Pfizer with Wyeth and Merck with Schering-Plough.
Megamergers might not be the answer this time, however. For one, current pharma executives have expressed reluctance to do big deals because of the complexity of combining two companies. There is debate, too, over the effects such deals have on market valuation and R&D productivity afterwards.
Another reason is that, after years of industry consolidation, there are not many major large drugmakers left as attractive merger targets. Those that remain have patent cliffs of their own, Goldstein said.
Instead, the hunt for new products will either be in big drugmakers’ own laboratories or in those of smaller biotechnology companies. By having two successor blockbusters already in waiting, AbbVie has shown it can execute on the former approach.
Yet, across the industry, big drugmakers’ “R&D productivity is not necessarily corresponding to the R&D investment,” Ural said. R&D productivity and returns have, with a few exceptions, steadily declined each year over the past decade, according to data from both IQVIA and Deloitte.
Meanwhile, in biotech, “there may not be enough assets out there,” Ural added. “It’s going to be a fight for established assets, of which there aren’t that many.”
That fight will be fueled by large cash holdings. Jefferies analyst Michael Yee estimates big drugmakers have $500 billion in cash to spend on acquisitions and other pipeline-building transactions. Small and mid-sized biotechs have simultaneously seen their valuations drop, limiting their financial options, Yee wrote in a Feb. 5 note to clients.
The experimental drugs large pharma companies chase, through acquisition, licensing or inside research, might need to be different, too. They could find advantages in development platforms that can generate multiple new medicines like messenger RNA, gene editing or next-generationantibody technology, or in drugs that have promise across multiple indications.
Humira-sized blockbusters may become harder to achieve, though, which will change how drugmakers develop and commercialize new products, said Bill Coyle, global head of biopharma at consulting firm ZS. AbbVie, for example, needs two drugs — Sykrizi and Rinvoq — to replace sales of Humira.
“I think we’re potentially entering an era of fewer blockbusters and a lot more smaller products,” he said. “The other shift for many of the big pharmas is that their cadence of launch needs to be more efficient and frequent. They need to become more effective launchers of new assets.”
Patent thicket-ing
For drugs further from patent expiration, extending the date of generic or biosimilar entry through the construction of a “patent thicket” is another tactic drugmakers are pursuing. By surrounding Humira with dozens of patents in the U.S., for example, AbbVie pushed off biosimilar entry by seven years after the drug’s principal patent expired.
Others in the industry are seeking to do the same. Merck is testing a subcutaneous version of the intravenous Keytruda, which could potentially merit a separate patent and extend its market exclusivity by years.
The intravenous form of Keytruda
Courtesy of Merck & Co.
While subcutaneous Keytruda would likely still be delivered by physicians, it could be more convenient. “It’s not the same as having to get an IV, where you have to sit in a chair for an hour or two,” Kelly said.
Other drugmakers sought to push out the entry of biosimilars using this strategy, including Johnson & Johnson with its multiple myeloma medicine Darzalex and Bristol Myers with its Keytruda rival Opdivo.
Already, Bristol Myers has benefited from such intellectual property practices with its medicine Revlimid. The blood cancer drug’s exclusivity was protected by patents held by its original developer, Celgene, that were strong enough to keep most generic competition at bay through 2026. That will give Revlimid, a small molecule drug, a pattern of sales decline that looks more similar to biologic drugs, at least for a few years.
Tahir Amin, founder and executive director of the Initiative for Medicines, Access & Knowledge and a critic of pharma companies’ intellectual property practices, said he expects drugmakers with approaching cliffs to use late-earned patents to delay competition.
Striking limited distribution deals with copycat drugmakers, as Celgene did with Revlimid, could also be a tactic to stave off government drug price negotiation, because the Inflation Reduction Act limits that authority to only those products with no competition.
“At the end of the day the patent system is going to define how they shape the market,” he said.
Article top image credit: Courtesy of AbbVie
A new, non-opioid pain drug is here. Getting it to patients could be agony.
After decades of research, Vertex Pharmaceuticals has an approved pain medicine. Can one of the most powerful biotechs contend with a healthcare system that’s long favored opioids?
By: Jacob Bell• Published Jan. 31, 2025
Editor’s note: This story was published Jan. 31, 2025, immediately following Journavx’s U.S. approval. Since then, Stuart Arbuckle, who served as Vertex’s chief commercial officer, has left the company.
For the last quarter century, one of the world’s most capable drug developers toiled to make a new, non-addictive kind of painkiller. The journey was fittingly excruciating.
Pain, as Vertex Pharmaceuticals found out, is wildly complex. It starts simple enough, with a sliced hand or burned finger or broken bone. But it convolutes fast. Special nerve cells, activated by potentially dozens of chemicals and proteins, sense the pain and launch a signal up the spine like a firework, lighting up a patchwork of brain regions that interprets this message and decides how the body will feel.
Much about how this process unfolds in any given person remains hazy. Scientists suspect genetics, past experiences and the environment each play some role, perhaps explaining why two people who suffer the same injuries can have such dissimilar pain. This intricate web tripped up many large pharmaceutical firms, a key reason why no truly innovative medicines have come forward in more than two decades.
Vertex was one of the few to trudge ahead. Its pain labs in San Diego discovered, fine-tuned and tested promising compound after promising compound. Invariably, though, studies would show them not safe or potent enough to meet Vertex’s exacting standards. Not until about 20 years into its hunt did the company find a molecule worth championing.
On Jan. 30, the Food and Drug Administration approved that molecule, now called Journavx, as a treatment for the sharp, short-lived “acute” pain usually felt after an accident or a surgery. Expectations around Journavx are high. With the U.S. still mired in an overdose crisis that’s killed hundreds of thousands of people, Vertex is positioning its medicine as a valuable alternative to opioid-based therapies.
Doctors say they’re eager to have another tool at their disposal. Wall Street views Journavx as a billion-dollar product.
Journavx has a real chance to “bend the curve on the opioid epidemic,” said Stuart Arbuckle, who, as Vertex’s chief operating officer, is overseeing the drug’s launch. “This is the first real alternative. The other is to leave these people in pain, and that's not an acceptable choice.”
Yet the true impact of Journavx will hinge on whether Vertex can contend with a healthcare system that favors the cheapest possible option — a system which, at the hands of drugmakers, insurance companies and pharmacy middlemen, was gamed for opioid use. Doctors across the country, from Oregon to West Virginia to Massachusetts, envision the biggest barrier to prescribing Journavx being insurers, as they tend to resist covering new, higher-cost pain drugs. Vertex set the medicine’s price at $31 a day, many times more expensive than generic opioids like hydrocodone.
Pain is unlike any other drug market, presenting both an opportunity and a challenge for Vertex. The least expensive therapies have ruined countless lives, and wreckage from the opioid epidemic has, for some time, prompted a shift to a layered treatment approach that tries to use these powerful drugs only as a last resort. Vertex’s mission is to convince doctors and insurers that Journavx belongs somewhere in the mix.
Arbuckle claims, as industry executives often do, that his team has had fruitful conversations with these stakeholders, that they appreciate Journavx may fill a major gap in pain management. They’ll need to for most patients to have a shot at accessing the drug.
“In some ways, talk is cheap,” Arbuckle said. “It really will depend on what we see from people in terms of action in the days and weeks following approval.”
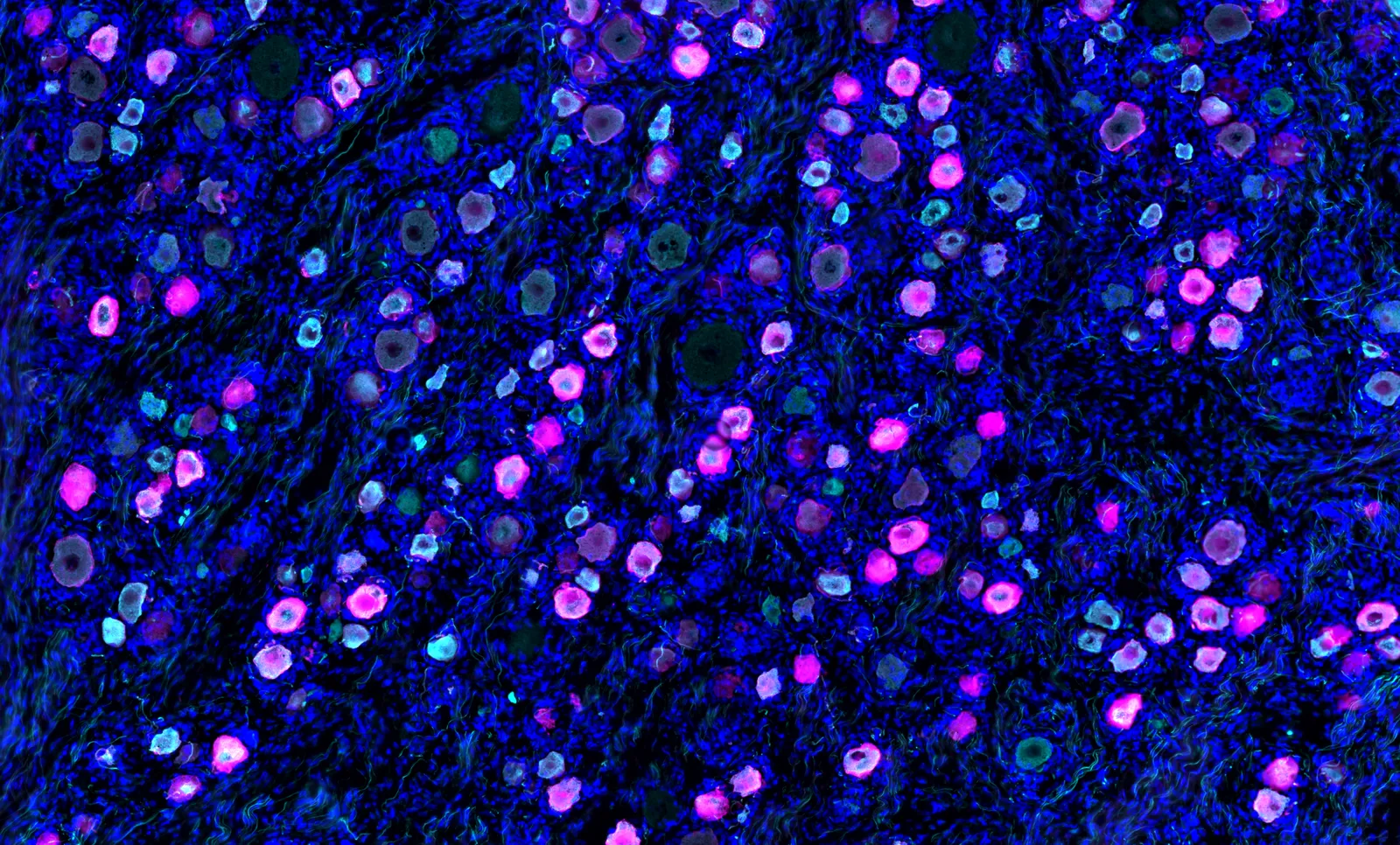
Journavx targets in peripheral nerve cells an ion channel called Nav1.8, colored magenta in this immunofluorescence image.
Permission granted by Nwasinachi Adriana Ezeji/Center for Advanced Pain Studies, University of Texas at Dallas
Debating value
Supporting Vertex’s case are a pair of large clinical trials that assessed Journavx in people who underwent either a “tummy tuck” or a bunion removal, two notoriously painful surgeries. Both experiments showed the drug was significantly better than a placebo at easing pain. It also worked decently fast. Participants reported some relief within a few hours.
Unlike all other approved pain drugs, Vertex’s blocks tube-shaped proteins found almost exclusively in nerve cells located outside the brain and spinal cord. These “NaV1.8” proteins act like cell towers, transmitting pain waves to the central nervous system. In addition to being effective, studies have found Journavx to be remarkably safe. It doesn’t appear to have the addictive qualities of opioids, which bribe the brain’s pleasure centers, and compared to a placebo it actually was associated with lower rates of common ailments like nausea, constipation and headache.
Vertex took these results and asked the FDA for a broad approval in moderate-to-severe acute pain. With that now in hand, Vertex can enter the segment of the pain market where opioids are more readily prescribed. The company has also been sponsoring research to expand into different types of chronic pain.
There, Journavx has delivered mixed results. Vertex lost $15 billion in market value in December when data from a lower back pain trial disappointed investors. A year earlier, however, a study focused on the chronic nerve pain caused by diabetes showed Journavx to be about as effective as the main ingredient in Lyrica. Analysts described that performance as “solid” and “strong.”
Journavx has other limitations. The two acute pain studies explored whether it is superior to a combination of Tylenol and a commonly prescribed opioid. On that measure the drug fell short, a “glaring” outcome for Richard Vaglienti, medical director of the Center for Integrative Pain Management at West Virginia University, which treats roughly 1,600 patients a month.
Vertex rejects that this finding will be a hangup. “Go and ask physicians and patients,” Arbuckle said, “they'll tell you that's not what they're looking for.”
Vertex did just that last year, commissioning a survey of around 550 healthcare providers and 1,000 adults recently treated for acute pain. Their bigger concerns, according to the company, were the addictive potential of opioids and the exigencies of having few non-opioid options.
Taken together, Vertex’s data have left many experts with a positive view of Journavx, yet no firm agreement on precisely which scenarios it is best suited for. Vaglienti thinks it’s “possible” the drug could have a “decent role to play” managing non-severe chronic pain, and might be particularly useful for patients who can’t tolerate more potent drugs.
Kimberly Mauer, vice chair of the pain center at Oregon Health & Science University, sees it as more widely applicable. “This sounds like an exciting option, because it's going to be opioid-like, and maybe not have the side effects or the risk,” she said. “And if it doesn't work as well as opiates, I'm OK with that. Because I can maybe pair it with something else.”
While drug research and opioid mitigation strategies often focus on chronic pain, having a pill like Vertex’s in the acute setting is “extraordinarily important,” said Theodore Price, director of the Center for Advanced Pain Studies at the University of Texas at Dallas. That’s because many people are susceptible to opioid addiction but don’t realize it until they’ve been prescribed the drugs following a trauma or operation.
Tens of millions of surgeries happen annually in the U.S. And while estimatesvary depending on the period studied, recent research indicates a large portion of surgery patients are still prescribed an opioid.
“There's nothing you could say that could convince me this doesn't have an impact on what happens to them later on in their life, at least some portion of them,” Price said.
Accidental overdoses involving an opioid remain high. Nearly 82,000 people in the U.S. died that way in 2022. Almost 15,000 of those deaths involved a prescription opioid. Price himself lost one of his best friends to an overdose about 15 years ago, after the friend was first exposed to opioids for pain management.
“It's a tragedy,” he said. “If we could have a drug that would help us to avoid this, it would be an absolutely massive benefit to humankind.”
Addiction treatment can help people with opioid use disorder, but researchers have found that insurance rules can limit access to medicines like buprenorphine.
Permission granted by OHSU/Kristyna Wentz-Graff
The price point
Jose Zeballos understands this need well. As an anesthesiologist and leader of the acute postoperative pain management service at Brigham and Women’s Hospital, Zeballos cares for hundreds of patients every year. A few advances in treatment have emerged during his tenure, like new, longer-lasting local anesthetics, but overall “nothing else has come out that really has helped.”
Vertex’s medicine could therefore be an “amazing” addition, he said, as it may offer some relief not only after surgery, but in everyday pain management as well. Journavx might dull persistent back aches or take the edge off a sports injury. And, since opioids can confuse and disorient, it could be an especially valuable alternative for elderly patients.
Despite the many use cases, Zeballos speculates that doctors will reach for Journavx only if it’s “easily accessible,” and that depends on insurance companies stomaching the drug’s price tag. “It probably all comes down to financials more than anything else.”
Arbuckle says price and access are by far the biggest issues brought up when Vertex’s commercial team discusses Journavx. Millions of prescriptions for acute pain are written every year in the U.S., so, from the payer perspective, “if you're seen millions of anything, you're worried about the budget impact.”
Generic opioids like hydrocodone cost less than $2 a day. Advil and Tylenol are cheaper still, making Journavx’s price of $31 a day high enough to draw close examination from insurers.
Arbuckle argues that’s the wrong comparison, since it doesn’t account for the devastation opioids bring to both the healthcare system and society at large. A report from the Congressional Joint Economic Committee tried to calculate this cost and, looking just at 2020, assessed the total at nearly $1.5 trillion, one-third higher than three years prior.
“This is not an academic, side-by-side, two things have equivalent efficacy and one's cheap and the other one isn't [exercise],” Arbuckle said. “Every time a physician and patient chooses [our drug] when they would previously have chosen an opioid, that is one less opportunity that person is exposed to the potential liabilities of opioids, gets opioid use disorder and becomes a horrible statistic.”
Vertex is beholden to investors as well as patients. The price set by the company may have societal value baked in, but it’s also meant to drive revenue. One analyst expects Vertex’s pain portfolio, which includes Journavx and a series of follow-on drugs already in development, could eventually generate north of $10 billion a year.
Analysts at the investment bank Cantor Fitzgerald recently spoke to a senior director of product development at one of the nation’s largest insurers, UnitedHealth Group. The director predicted Journavx will get broad coverage, as payers are under serious pressure to cover non-opioid medications.
He also doesn’t anticipate the drug will be subject to “step therapy,” a controversial insurer practice that requires patients to “fail” on cheaper drugs before trying newer, pricier medicines.
Optum, a pharmacy benefit manager owned by UnitedHealth Group, declined to answer BioPharma Dive questions on its coverage plans for Journavx. Insurers Humana, Cigna and CVS Health did not respond to requests for comment. Vertex has talked to payers as well as parties that “paid billions of dollars for their role in the opioid epidemic,” according to Arbuckle, and the conversations have been “really positive.”
“Virtually everybody we speak to totally gets it,” he said. “Does that mean we're going to have tough negotiations on price? Of course. Do we think we’ll have to negotiate access? Of course. Do we have to go through formulary procedures? Of course. But it's not like we're getting a stiff arm from people.”
If Vertex does get payer buy-in, Journavx could be an exception to a longstanding, unwritten rule in pain management: fresh therapies take a while to reach patients. One of the company’s immediate goals is to cut down this timeline and to make sure, if patients are prescribed Journavx, they can pick it up over the counter at their local pharmacy.
At OHSU’s pain clinic, Mauer said her team rarely uses new medications within months of them coming to market, because insurers haven’t yet decided coverage plans and the out-of-pocket costs are too high for most patients. Nine times out of 10 the wait is “pretty long.”
“The problem with any new drug is the reluctance of insurance companies to pay for it because of the heavy upfront cost,” Vaglienti said. “So even though there are risks with opioids, from the insurance company side, 30 Percocet really only costs a few dollars.”
Vertex Pharmaceuticals researchers work in the company's San Diego laboratories.
Courtesy of Vertex Pharmaceuticals
A turning tide
Journavx, then, may serve as a proving point for Vertex. The Boston-based biotechnology company has grown to an almost $115 billion valuation by selling big-ticket medicines for uncommon diseases with few to no other remedies. Pain has a trove of generic treatments and, just in the acute setting, Vertex approximates 80 million adults in the U.S. are prescribed a medicine each year.
Pricing barriers like the ones facing Journavx can be overcome, though success often takes time. Between 2018 and 2020, a novel class of injectable migraine drugs came onto a market flush with generics. While one is now approaching blockbuster status — $1 billion or more in annual sales — the others remain only modestly successful. A similar dynamic awaits a new schizophrenia treatment from Bristol Myers Squibb, which, while pegged for success, faces numerous, lower-cost competitors.
Journavx’s launch comes at what might be considered an opportune time. The reckoning over opioids still lingers in the public eye. In January, members of the Sackler family and Purdue Pharma agreed to pay as much as $7.4 billion in a revised legal settlement over the OxyContin maker’s role in the epidemic.
Federal and state lawmakers are also taking action. Two Congressional bills — one enacted in January, the other introduced in the Senate last year — aim to amend Medicare so older Americans can more easily access and afford a list of certain non-opioid pain medications. Journavx is eligible to join this list, though it likely won’t be added until at least 2026.
Policies like these could help “level the playing field” in the pain market, Arbuckle said, and their arrival represents a “turn in the tide.”
The executive is adamant that Vertex can make the most of this momentum. It’s been preparing for Journavx’s approval for “a number of years now,” he said, and amassed 150 staff to sell it.
Still, there are doubts the launch will go as smoothly as Vertex — or its investors — might hope.
RBC Capital Markets analyst Brian Abrahams is braced for “limited initial adoption” and thinks the $90 million figure that other analysts have forecast for 2025 sales is “optimistic.” Paul Matteis of Stifel shares those reservations. In acute care, he said, "it's almost impossible to find a good drug launch" for anything non-lifesaving, in large part because the field "moves really slow" to adopt new treatments.
Both analysts note that, for Journavx to hit that $90 million mark, hundreds of thousands of patients would need to take the drug. "No one has a clue how to model it," Matteis said.
The medical and research communities may be holding their breath, too. Price, of the University of Texas, fears that if Vertex doesn’t make a strong enough case, it could dampen enthusiasm around Journavx or even broader pain research.
“Any medication that is effective for treating pain of any type, that doesn't have all the negative things associated with opioid therapy, would be extremely valuable,” said Vaglienti. “And I know the company is probably banking on this being one of those medications. That will remain to be seen.”
Article top image credit: Permission granted by Vertex Pharmaceuticals
The state of drug pricing in 2025
In February, the U.S. government put forward its initial price proposals on 10 top-selling medicines, kicking off negotiations that will run through September. Drugmakers argue the process is price-setting, rather than a negotiation, and have warned the law will jeopardize biomedical innovation.
included in this trendline
Trump redoubles threats in attempt to strongarm drugmakers on prices
Pharma prepared to work with Trump on DTC drug sales: Pfizer CEO
Ozempic, Ibrance among next drugs picked by Medicare for price talks
Our Trendlines go deep on the biggest trends. These special reports, produced by our team of award-winning journalists, help business leaders understand how their industries are changing.