This feature is part of a series focused on Alzheimer's disease. To view other posts in the series, check out the spotlight page.
Alzheimer’s disease is one of the top ten leading causes of death in the U.S., affecting more and more Americans as the country’s population ages. But of the leading causes of death, it's the only one that lacks an effective treatment for preventing, slowing or curing the memory-robbing neurodegenerative condition.
Despite the pharma industry’s best efforts, promising drug after promising drug have failed to show an ability to improve cognitive function or otherwise alter the course of disease. Nevertheless, both big pharma and biotechs continue to invest millions in hopes of uncovering a breakthrough.
Past failures shape the current drug development landscape, but so too do the lessons imparted by those setbacks. Underpinning both is a growing need that continues to incentivize drugmaker R&D.
1) Continued investment despite failure
In the decade from 2002 and 2012, only one compound out of 244 studied in clinical trials reached markets in the U.S., making for a dismal overall attrition rate of 99.6%. That represents one of the lowest marks for any therapeutic area, according to the oft-cited study which documented the string of clinical failures.
No disease-modifying treatments have been approved to date and only a handful of symptomatic therapies are OK’d for use in the U.S.
Recent high-profile failures from Eli Lilly’s experimental monoclonal antibody solanezumab and Merck’s BACE inhibitor verubecestat have only served to continue that trend.
But despite hundreds of misses, the industry continues to invest in expensive clinical development in hopes to striking it big with a disease-modifying Alzheimer’s drug.
More than a hundred candidates are in development across the industry, according to a recent study, and pharmas continue to ink new deals to gain access to emerging science. Irish pharma Allergan, for example, paid $125 million last November to acquire Chase Pharmaceuticals and gain access to its Phase 2 Alzheimer’s candidate.
Biogen's experimental antibody aducanumab, meanwhile, has taken up the mantle as the next greatest hope for a breakthrough. Trials for that drug are expected to read out starting in 2019.
Even those companies that have been burned in the past have shown a dogged staying power. Eli Lilly says its remains committed to Alzheimer’s despite solanezumab’s disappointment and recently broadened its collaboration with AstraZeneca to include a second drug.
Merck, while defeated in its EPOCH study of verubecestat, will continue its APECS trial of the drug in prodromal patients.
Some of this can be chalked up to inertia, pushing on with development started years before. But the potential market opportunity and unmet medical need continue to attract companies willing to bet on the progress of science.
2) Rising prevalence, rising cost
Already impacting the lives of five and a half million U.S. adults, Alzheimer’s could affect as many as 13.8 million adults over the age of 65 by 2050 as the population ages more rapidly, according to the the Alzheimer’s Association.
With no disease-modifying treatments in the pharmaceutical armamentarium, the number of deaths from the neurodegenerative disease will also rise. The age-adjusted rate of deaths per 100,000 people rose nearly 55% between 1999 and 2014, according to the Centers for Disease Control and Prevention.
Increased prevalence will exert a sharp pressure on healthcare costs, both direct and indirect.
The total cost of care (including uncompensated care) for patients with Alzheimer’s and other related dementias will hit an estimated $259 billion this year and rise to a staggering $1.1 trillion by 2050, according to the Alzheimer’s Association.
Put it together and winning approval for a successful disease-modifying treatment would be a mega-blockbuster opportunity.
A white paper put together by the healthcare services firm QuintilesIMS estimates a monoclonal antibody priced at $18,500 per patient year would result in $30 billion in drug costs if used in clinical Alzheimer’s patients in the U.S. Adding in prodromal patients would push that figure as high as $55 billion.
3) Aiming drug development earlier
Eli Lilly’s clinical setback last fall with solanezumab wasn’t the first time the Indianapolis drugmaker has come up short trying to prove that particular drug’s benefit.
Two prior Phase 3 studies of solanezumab — Expedition 1 and Expedition 2 — had failed to show an improvement over placebo in patients with mild-to-moderate Alzheimer’s. Analyzing the trial results, however, Lilly thought it had detected a positive impact on cognition in patients only with mild forms of the disease. Re-energized, the drugmaker fired up another pivotal study to chase down that hope.
Although that attempt failed, the drive to look earlier in treating Alzheimer’s remains a prevailing strategy in clinical development of new treatments. Those past clinical blow-ups are also expanding understanding of the disease, providing useful evidence for future research.
"A lot of what we know today is the result of past failures."
Rupa Doshi
Senior director of neuroscience clinical strategy, inVentiv Health
"A lot of what we know today is the result of past failures," explains Rupa Doshi, a senior director of neuroscience clinical strategy at inVentiv Health, a contract research organization and consultancy.
What the disappointing setbacks of solanezumab and verubecestat (and others before them) have shown is that testing drugs in patients with mild-to-moderate Alzheimer’s likely comes too late.
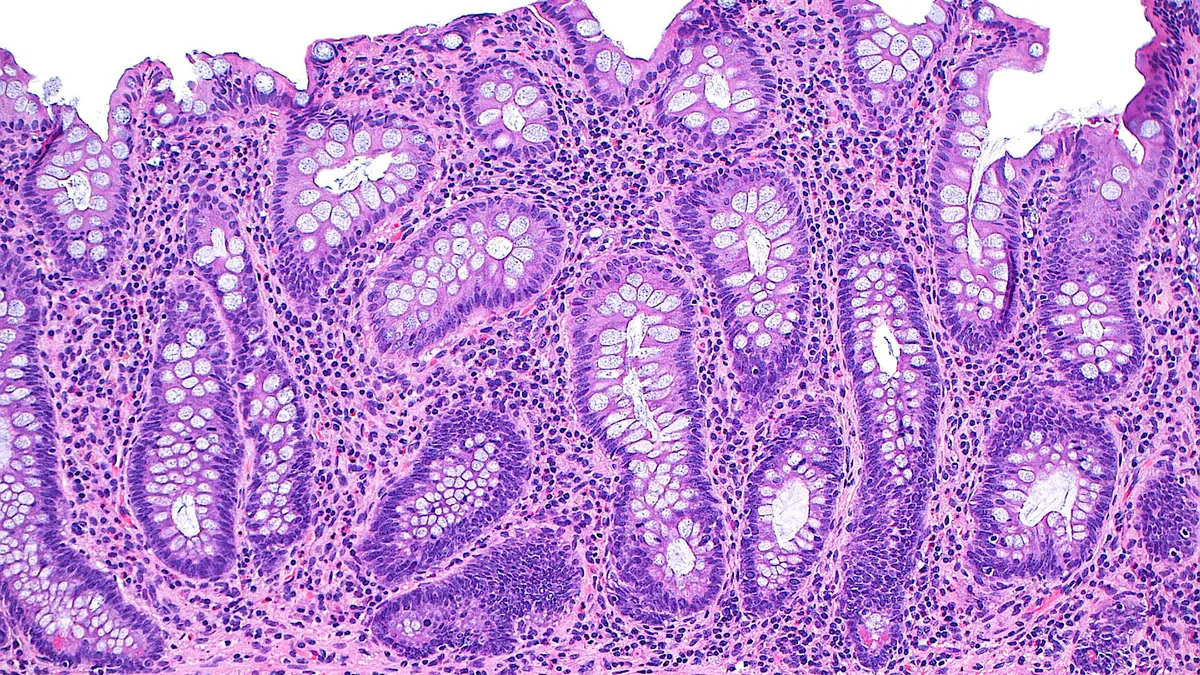
Research suggests that changes in brain structure, such as the formation of amyloid plaques, may have begun developing a decade or more before cognitive decline and diagnosis.
"I think we should recognize that even if you have mild Alzheimer’s disease, your brain has been accumulating amyloids for decades, and you almost have maximum amyloid in your brain already," said Jan Lundberg, head of Eli Lilly’s Research Laboratories, on a call with investors in January.
Trying to treat Alzheimer’s after the damage has been done, in other words, is unlikely to yield a game-changing treatment.
"Prevention is now the new frontier," Doshi says, pointing towards prodromal and at-risk patient populations.
4) Doubling down on biomarkers
Shifting earlier and earlier in Alzheimer’s may yet yield dividends, but such a strategy also presents new hurdles, such as reliably identifying and recruiting patients for clinical trials.
Patients with prodromal Alzheimer’s or mild cognitive impairment may go undiagnosed until symptoms manifest themselves more severely, for example.
Adding to that challenge, genetic mutations account for only a small percentage of total cases of Alzheimer’s. Most cases are sporadic, making it more difficult to identify patients at higher risk of developing the disease before some of the pathological signs or symptoms begin to show up.
That being said, a good deal of progress has been made in better understanding potential risk factors and in screening patients for inclusion in clinical trials.
"When it comes to research, we are able to select the patient population better than we could in the past," says inVentiv’s Doshi.
Positron emission tomography (PET) imaging for the telltale clumps of amyloid plaques has improved, as has the ability to detect amyloid levels in cerebrospinal fluid (CSF). More clinical trials now require evidence of such plaques as a criterion for inclusion.
Half of currently ongoing Phase 3 studies and nearly 30% of Phase 2 trials for disease-modifying Alzheimer’s treatments are gated based on either CSF or PET testing for amyloid, according to data from a recently published study by researchers at the Cleveland Clinic.
Past failures in clinical development, such as the first Phase 3 trials of solanezumab, appear to have been hamstrung by inclusion of patients diagnosed with Alzheimer’s but who lacked positive testing for amyloid.
Improved patient selection, in theory, should help better match targeted therapies with the correct patients. In addition, better diagnostic capabilities should help clinical researchers measure smaller changes — important in earlier patient populations.
"We're trying to jump ahead and we're failing."
Michael Sasner
Research scientist, The Jackson Laboratory
But more work needs to be done. "We're trying to jump ahead [in clinical testing] and we're failing because we don't have the foundation yet in terms of understanding the brain, understanding the disease, understanding the models that we are using," notes Michael Sasner, a research scientist at The Jackson Laboratory Alzheimer’s Disease Center.
JAX — as the lab is better known — is working to develop more predictive mouse models that better simulate the actual patient populations biopharma companies are testing drugs in.
5) Widening the focus
One of the big questions in light of recent failures of high-profile amyloid targeting drugs is whether the setbacks undermine the underlying hypothesis behind going after amyloid plaques.
Researchers and pharma executives have largely argued this is not yet the case. Lilly’s Lundberg has said it remains too early to tell whether clinical results have disproven the amyloid approach, pointing to the clear indications of amyloid’s involvement in disease pathology and to the continued difficulty of getting enough drug through to the brain.
For inVentiv’s Doshi, the amyloid hypothesis is still here to stay. But she also noted the promise of other targets, such as the tangles of protein fibers called tau that are seen in Alzheimer’s patients. Anti-tau drugs have failed as well, though combinations of the two approaches could offer new opportunities.
Other mechanisms of action currently under study include targeting inflammation and metabolic pathways.
Greater diversity of research into different approaches could help fuel new progress. Sixteen of the 18 disease-modifying treatments counted as being in Phase 3 by the Cleveland Clinic study are aimed at amyloid or tau targets.
Yet only 19 of the 36 disease-modifying drugs in Phase 2 target amyloid. Seventeen are being developed using differing mechanisms of actions, suggesting new approaches are beginning to emerge. And while earlier-stage testing still has its share of amyloid drugs, this greater diversity of approaches down the pipeline could shed light on what’s missing from the amyloid-alone approach.
More work is also ongoing to better understand risk factors for Alzheimer’s, such as the apolipoprotein E (APOE) 4 gene.