Over the last five years, the pharmaceutical industry has brought to market a series of first-of-their-kind treatments for some of the most devastating brain disorders. The list includes Cobenfy, a schizophrenia drug that Bristol Myers Squibb spent $14 billion to acquire; Qalsody, a genetic medicine designed for a small subset of the ALS population; and a trio of therapies from Eisai, Biogen and Eli Lilly that each target the sticky, toxic plaques many researchers believe to be the root cause of Alzheimer's disease.
Scientific advances continue to pile up. One branch of research, focused on tube-shaped proteins known as ion channels, is progressing so rapidly that some expect it to produce new therapies for epilepsy and mood disorders in the coming years. Vertex Pharmaceuticals, which helped pioneer the study of these channels in relation to pain, recently succeeded in a decadeslong mission to bring a new, non-opioid medication to patients. Wall Street analysts called the medication's approval a "watershed" moment for pain research.
These victories only tell half the story of neuroscience, however. Because while this field has allured some of the world's brightest minds and most powerful drug companies, its complexities have also brought copious hard-felt setbacks. Brain research continues to be branded as "high-risk, high-reward," a moniker that has discouraged many developers from making it a core part of their businesses. To that end, British pharma giant AstraZeneca quietly exited the space in 2025.
Amid this push and pull, money has kept pouring in. Novartis, GSK, AbbVie, Biogen and Roche have each inked fresh, neurology-focused deals. So did Johnson & Johnson, which agreed to spend $15 billion on psychiatry specialist Intra-Cellular Therapies.
Additionally, neuroscience remains one of the more favored therapeutic areas for early-stage investors and biotech creators. It received more than $1.7 billion in venture money in 2025, across more than two dozen of the industry's most prolific firms. A report from Silicon Valley Bank found venture capital investment in U.S.- and European-based neurology companies has risen north of 20% since 2022.
Read on for a closer look at how this field is evolving:
In AbbVie deal, Wall Street sees momentum for psychedelics M&A
A billion-dollar acquisition of Gilgamesh Pharmaceuticals suggests big pharma may finally be willing to place significant bets on psychedelic research.
By: Jacob Bell• Published July 31, 2025
Biotechnology companies specializing in psychedelics research saw their share prices rise after rumors of a billion-dollar acquisition hinted that big pharma is now more open to betting on this area of drug development.
Bloomberg News reported in July that AbbVie was in talks to buy privately held Gilgamesh Pharmaceuticals. The deal, formally announced a month later, handed AbbVie a small slate of experimental therapies for depression, anxiety and mental health conditions. Gilgamesh’s most advanced drug, code-named GM-2505, works by latching onto a brain protein known to interact with psychedelics like LSD and psilocybin.
Prior to the deal, Gilgamesh’s possible takeover appeared to have buoyed investor confidence in psychedelics companies. Shares of multiple biotechs, including Atai Life Sciences, Compass Pathways, Cybin, Mind Medicine and GH Research all benefitted.
Joshua Schimmer, an analyst at the investment bank Cantor Fitzgerald, said he wasn’t surprised to see big pharma taking more interest in psychedelics, since these therapies have shown “transformational” potential across a range of mental health disorders. Compass, for one, in June announced results from a late-stage clinical trial wherein a single dose of its psilocybin therapy significantly reduced symptoms of treatment-resistant depression.
Gilgamesh also disclosed in May 2025 positive results from a study of GM-2505, which, according to the company, was able to quickly, effectively and durably treat the most common form of depression.
“This is one of the most important waves of innovation we're seeing today in biotech,” Schimmer said. “We need more clinical data readouts in proper, large, randomized, controlled trials. But so far, we're seeing things we've really not seen before in psychiatric care, and it doesn't end with depression.”
Analysts noted, too, the inroads psychedelics are making with drug regulators. Martin Makary, commissioner of the Food and Drug Administration, and Robert F. Kennedy Jr., head of the Department of Health and Human Services, both support speeding up the testing — and possible approval — of psychedelics. The FDA, under former president Joe Biden, also issued guidance in 2023 for psychedelic drug developers.
“The macro backdrop continues to improve,” wrote Jefferies analyst Andrew Tsai in a note to clients. Tsai added that a Gilgamesh purchase, should it happen under the alleged terms, would be larger than previous deals for these kinds of assets. That could help assure Wall Street that psychedelics are “an investable space.”
Additionally, concerns raised by the 2024 flame-out of one of the field's leading players, Lykos Therapeutics, have since eased. Analysts view the problems that company encountered in its attempt to win approval of MDMA-assisted psychotherapy as unique.
While those tailwinds can help catalyze bigger-ticket acquisitions, there are reasons to believe such deals won’t come easily. For instance, many of the deepest-pocketed drug firms have found neuroscience too risky and backed away from it over the years. That aversion, if it persists, could keep the pool of potential buyers narrow.
Psychedelic developers may also not be so keen to come to the negotiating table, especially since medium-sized companies like Intra-Cellular Therapies, Axsome Therapeutics and Acadia Pharmaceuticals have demonstrated that brain drugs can be successfully commercialized without big pharma resources.
Many of the current crop of psychedelics biotechs have “very strong management teams” with considerable experience selling medicines, Schimmer said. “I don't see why you need a large pharma company to get this done.”
Kabir Nath, CEO of Compass, told BioPharma Dive in mid-2025 that his team isn’t designing the company to be sold. The focus, rather, is getting Compass’ psilocybin therapy through the final stages of testing and onto the market.
“It's very exciting to see the resurgence of interest in psychiatry in general, from big pharma and so on,” he said, but “we can't expect to be bought or partnered.”
“Like any board, if somebody comes knocking at the right point, we'll have the discussion,” Nath added. “The door is not closed.”
AbbVie has been more active than many of its peers inking deals that revolve around the brain. In late 2023, the company agreed to spend almost $9 billion to take control of Cerevel Therapeutics and a once-promising schizophrenia therapy.
Since then it dropped $1.4 billion on a Johnson & Johnson-backed startup built around a type of brain drug technology. Then, it took a $355 million stake in a biotech developing genetic medicines for neurological disorders, among other diseases.
The Gilgamesh acquisition further diversified the company’s neuroscience research while thrusting it into a field few other large pharmaceutical firms have felt comfortable dedicating significant resources to. J&J is the main exception there. It already sells Spravato, a form of ketamine that’s used to treat depression and generated more than $1 billion in 2024.
J&J has also closed its $15 billion purchase of Intra-Cellular, providing access to a lucrative, mind-stabilizing drug called Caplyta as well as a series of experimental, non-hallucinogenic psychedelics.
In a report, analysts at RBC Capital Markets argued the psychedelic space is “approaching a tipping point” as late-stage readouts near and Spravato gets on track to deliver $2 billion in yearly sales. Spravato has “increasingly validated the market,” according to the report.
Gavin Clark-Gartner, an analyst at Evercore ISI, agrees the Spravato story has been a major force toward de-risking psychedelic drug research. However, he cautions that the biotechs coming up in the space will likely have to build upon the commercial infrastructure J&J laid.
“It is not necessarily flipping a switch and a one-for-one translation from Spravato to a lot of these other therapies,” he said.
Article top image credit: Alamy
Psychiatry drugs finally have pharma’s attention. Can they keep it?
Recent biotechnology acquisitions have put emerging schizophrenia treatments in focus. But many development hurdles still stand in the way of new medicines for the brain.
By: Jacob Bell• Published April 8, 2024
Editor’s note: This story was published in April 2024 and has been lightly updated, most notably by referencing the approval of Bristol Myers Squibb’s Cobenfy, which was previously referred to as KarXT.
Even for the most deep-pocketed drug companies, $14 billion dollars is no small investment. That kind of money can buy large manufacturing plants, offices in glossy skyscrapers and entire campuses dedicated to specific research. But Bristol Myers Squibb has different plans.
Late in 2023, the pharmaceutical giant agreed to spend that much acquiring Karuna Therapeutics, a Boston-based biotechnology company. Karuna’s most advanced medicine later won U.S. approval as aschizophrenia treatment, bringing to market for the first time in decades a new form of antipsychotic. Some Wall Street analysts expect the drug to become a megablockbuster.
Bristol Myers sees significant opportunity too, though not yet enough to make psychiatry a top priority. “Failure rates are still very high,” noted Richard Hargreaves, who leads the company’s main neuroscience research center. “That was one of the reasons why neuropsychiatry moved into the biotech industry.”
“The bigger players like Bristol Myers, we watch how [biotechs’ efforts] unfold without actually dedicating big resources ourselves,” he said. “Personally, I'm not seeing us changing from [that] strategy.”
Once a cornerstone of large pharmaceutical firms, psychiatric drugs have been passed over for much of the last 20 years. Developers and investors gave various reasons for the collective retreat, but their decisions ultimately came down to dollars and cents math. Brain research had become too difficult, expensive and risky, and easier money could be made elsewhere.
The pullback has left a void of novel treatments for the hundreds of millions of people with conditions like schizophrenia, depression and substance use disorder.
Now, for the first time in ages, neuropsychiatry is back in focus thanks to the acquisition of Karuna, the potential approval of its medicine, as well as a $9 billion proposal from AbbVie to buy Cerevel Therapeutics, a company working on a similar schizophrenia therapy. While doctors and researchers welcome the excitement and argue it’s necessary to propel the field forward, they also wonder whether the renewed investment will be short-lived, as many of the issues that historically held back this area of drug development remain unresolved.
“The past is a very good predictor of the future,” said Paul Kenny, chair of the neuroscience department and director of the Drug Discovery Institute at Mount Sinai’s Icahn School of Medicine. “I think pharma will likely remain skeptical and trepidatious, because that's been the case for at least the past 10 years.”
“I don't know what's going to change that,” Kenny said. “Something big would need to happen.”
The dendritic tree of a Purkinje neuron is stained with the Golgi method.
Jose Luis Calvin Martin, Jose Enrique Garcia-Maurino Muzquiz via Getty Images
Cracking the brain
In many ways, the brain seems straight out of science fiction. A mass of 85 billion nerve cells acts as the body’s control center, directing everything from mood, movement and the senses to how we think, dream and problem solve. It’s the organ that “makes us human.”
Unsurprisingly, it’s also the most complex. In, 2023 an international team of scientists identified north of 3,300 cell types in the brain.
Researchers are “only scratching the surface in terms of our understanding,” according to Kenny. “Basically, every week, a new paper comes out [showing us] how cells are wired in ways that we didn't understand before, how they're functioning in ways that we just didn't appreciate.”
For drugmakers, this lack of understanding has brought costly setbacks. In Alzheimer’s disease, companies like Eli Lilly, Roche and Biogen each spent hundreds of millions of dollars investigating medicines that were ultimately unsuccessful in big clinical trials. And in ALS, more than half a dozen potential treatments flunked key studies over the past few years.
In neuropsychiatry, failures are so commonplace that finding new therapies has become, as an article recently published by Nature highlights, “the purview of only a handful of smaller more risk-taking biotech companies and a few academic drug discovery programs.” Karuna is one such example, as its “KarXT” schizophrenia medication is made from a molecule Lilly discarded years ago.
While all drug development is expensive and time-consuming, with very slim odds of success, the challenges are acute in neuropsychiatry. Researchers believe mood and behavior disorders are likely caused by small contributions from a constellation of genes, rather than just one or two faulty DNA sequences. Those tangled roots make choices around which proteins or molecules to target much harder.
Once a target is selected, drugs are designed and then tested in animals to anticipate how they’ll work in people. But these “models” are less reliable in psychiatry, since they assume animals and humans similarly express complex emotions and behaviors. In a mouse, it’s easy enough to see whether a therapy shrinks a tumor or reduces swelling. It’s much more difficult to tell if a mouse's anxiety resembles what a person might feel, or whether such stresses can build into something akin to depression.
“Scientists like me have a lot to answer for,” Kenny said. “We took animal procedures and extrapolated into humans far too readily.”
With such a shaky foundation, psychiatry drug programs tend to fall apart once they move into humans. Most other areas of clinical research are at least able to lean on biological markers that, much like car dashboards do for drivers, signal what’s going on in the body. But scientists have discovered relatively few of these for brain drug development in general, and next tonone in psychiatry.
That’s forced clinicians to rely on subjective assessments like surveys and questionnaires, which can be a particular problem in the large, placebo-controlled trials that are the gold standard of drug testing. Over the years, a laundry list ofpromisingtreatments for depression and other mood disorders fell short because patients in control groups did better than expected.
Psychiatry studies are “notoriously difficult to do, because you're trying to do everything you can to minimize a placebo response,” said Graig Suvannavejh, an analyst at Mizuho Securities who formerly held business development roles at AbbVie, Biogen and the biotech Alzheon.
“A lot goes into hopefully getting a high-quality trial outcome,” he said. “But in psychiatry, the variables are such that you can try so hard but still not know what you're going to get.”
The task for trial designers is made more complicated by the fact that diagnosing these diseases isn’t straightforward.
People with schizophrenia, for instance, can display a wide array of symptoms, from “positive” ones like hallucinations to “negative” ones like lack of motivation. Simultaneously, they may have other conditions like post-traumatic stress disorder, or be unable to consent and adhere to study rules.
“If somebody has just schizophrenia, that would be the most ideal, clean participant,” said Carol Lim, a psychiatrist at Massachusetts General Hospital. “In reality … it's a whole spectrum. If you have 1,000 people with schizophrenia, everyone will look different.”
Altogether, the pitfalls and obstacles have given psychiatry drug development an ominous reputation, with some experts describing an impassable chasm between the early science of their labs and the medicines pharma companies want.
Little progress has been made navigating this metaphorical gorge, which is why the KarXT story is so extraordinary.
Paul Kenny, chair of Mount Sinai’s neuroscience department, works with a researcher in a laboratory.
Permission granted by Mount Sinai
Finding something new
The journey of KarXT is well documented, as it represents not only a rare win in an exceedingly tough field, but also how central a role luck has played in the discovery of antipsychotics.
In the 1990s, Lilly was exploring whether a drug called xanomeline could improve cognition in Alzheimer’s patients. A nearly 350-person trial showed it had a modest impact. But more surprisingly, researchers noticed the drug seemed to quell the disruptive behavior and psychotic symptoms that often accompany Alzheimer’s.
The findings were especially alluring because xanomeline wasn’t like available antipsychotics — all of which block dopamine, a chemical brain cells need to communicate but is thought to trigger psychosis when in excess. Instead, Lilly’s drug worked primarily by boosting certain “muscarinic receptors,” proteins that are found throughout the body and interact with a different neurotransmitter, acetylcholine.
Though effective, dopamine inhibitors frequently cause weight gain, sedation and other health issues that lead patients to switch medications or stop taking them altogether. A more tolerable option could be highly valuable, so Lilly, intrigued by what the researchers had seen, set up a separate study with a small number of schizophrenia patients.
Again, xanomeline had a positive impact on psychosis. But its reach extended beyond the brain and into the gut, where it caused digestive problems. Because of these side effects, Lilly ultimately shelved the drug until 2012, when Karuna licensed it for the paltry sum of $100,000.
Andrew Miller
Courtesy of Karuna Therapeutics
Karuna had hatched three years earlier as the brainchild of Andrew Miller, who was at the time an executive at PureTech Health, the biotech startup creator that got Karuna off the ground. Miller believed xanomeline could still work; it just needed to be coupled with a drug that hindered muscarinic activity outside of the brain. The Karuna team found such a drug, and named the pairing KarXT.
"There was a huge amount of skepticism," PureTech CEO Daphne Zohar said. "Probably 100 investors passed on the idea."
Yet, since 2019, the therapy has succeeded in three medium to large clinical trials. Not only did KarXT significantly decrease the severity of schizophrenia symptoms, it didn’t cause excessive weight gain, restlessness or movement issues, though there were other side effects. The drug was approved by the FDA as Cobenfy in September 2024.
While there have been some innovations in antipsychotics, such as longer-acting shots, KarXT is viewed as a leap forward. “For the first time in 30 years you're seeing novel mechanisms now coming to fruition,” Hargreaves said.
At Mass General, Lim has found patients come to appointments asking about KarXT and eager to try it, based on what they’ve heard about it being effective without causing weight gain.
“It's the first time we're not directly targeting dopamine receptors. So we are avoiding a lot of side effects. That’s a really good thing,” Lim said.
In spite of the anticipation, doctors aren’t sure how much this milestone will actually benefit patients. They note how, in those KarXT studies, the main treatment periods lasted only five weeks and never pitted the drug against another antipsychotic. They’ve also said that, outside the tight controls of a clinical trial, patients might not find KarXT as effective or as easy to stay on.
How readily insurance providers would cover a drug like Karuna’s is another unknown, given the FDA has approved nearly two dozen antipsychotics, many of which have inexpensive generic versions.
“There's so much we don't know in terms of practical usage,” said Mitzi Gonzales, a neuropsychologist and director of translational research at Cedars-Sinai. “You really have to be sure it's better than everything else out there that's cheaper and more readily available.”
Jeffrey Lieberman, a psychiatry professor at the Columbia University Medical Center and a former member of Karuna’s scientific advisory board, foresees KarXT being a “huge” product initially. From there, physicians will closely watch how well the drug works, and whether it can meet their patients’ lofty expectations.
On Wall Street, expectations are equally high. Analysts at the investment firm Cantor Fitzgerald predicted KarXT sales will reach $1 billion a year starting in 2026, while Stifel analyst Paul Matteis has estimated peak annual sales will top $10 billion.
Matteis has also said three other companies advancing muscarinic receptor drugs — Neurocrine Biosciences, Neumora Therapeutics and MapLight Therapeutics — could see more interest from dealmakers in the wake of the Karuna and Cerevel acquisitions.
“The fact that they're just such a completely different mechanism and the majority of schizophrenia patients aren't well controlled, that can lead these drugs to being a really big class,” Matteis said.
KarXT works by stimulating a protein receptor that interacts with the neurotransmitter acetylcholine.
koto_feja via Getty Images
Building the pipeline
Beyond muscarinics, a handful of other drug classes are drawing attention back to neuropsychiatry.
Stimulating “orexin” proteins has been shown to help patients with narcolepsy, so companies like Takeda Pharmaceutical, Jazz Pharmaceuticals and Alkermes are trying to speed orexin-targeting medications to market.
Another group of proteins known as “TAARs” are seen as promising targets for treating schizophrenia and other psychoses. The most advanced of these drugs, from the Japanese developers Sumitomo Pharma and Otsuka Pharmaceutical, was recently evaluated across two late-stage clinical trials, but failed to meet the main goals of either.
A gene named TRPC encodes for proteins involved in nerve cell function, and research hassuggested inhibiting two of those may be helpful in a variety of psychiatric conditions. German drugmaker Boehringer Ingelheim is testing this hypothesis with a medicine in mid-stage testing for PTSD and major depression. Karuna is invested, too, having acquired exclusive rights to experimental therapies from the now-defunct Goldfinch Bio.
Drug hunters are also revisiting a well-known family of proteins that affects stress, mood and pain. Earlier attempts to regulate these “kappa opioid receptors” led to therapies that were held back by side effects. Cerevel, Johnson & Johnson and Neumora are developing new versions for the treatment of major depression that they designed to be safer.
Last summer, the FDA issued initial guidance for drugmakers interested in this research — a pool that has expanded considerably since 2019, when the agency granted a first-of-its-kind approval to a derivative of ketamine that J&J developed for depression.
Envisioning big returns, investors have been pouring money into psychedelic-focused biotechs. Bristol Myers’ Hargreaves expects the psychedelic field to advance as more drugs get cleared for human testing. “We’ll find new approaches into neuropsychiatry that way, I think as much as anything else.”
On a broader scale, Suvannavejh feels as though he’s seeing an increase in the number of mid- to late-stage trials for psychiatry drugs. The data is “pretty rich” compared to prior years, he said.
Still, psychiatry continues to make up a fraction of clinical research. A recent report from Iqvia, a healthcare services and information provider, found neurology accounted for 10% of all human studies started in 2023. There were around 60 in both schizophrenia and depression, and far fewer in anxiety and sleep disorders.
“I don't think the pipeline should be as empty as it is, based on our really burgeoning understanding [of the brain],” Kenny said. “We're really feeling the pinch, in the sense that those pipelines don't really exist.”
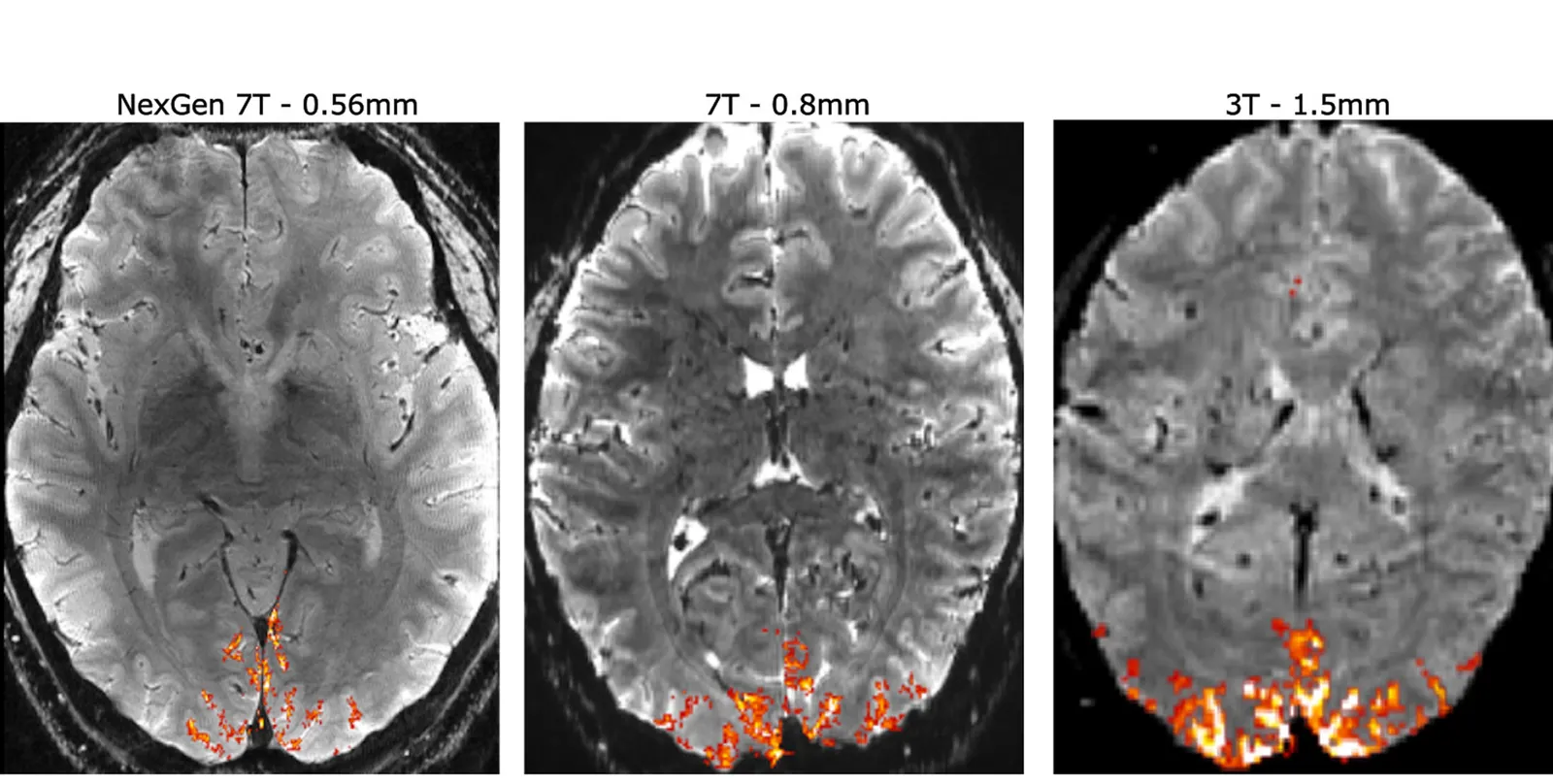
A comparison of human brain scans using high-resolution MRI technique versus standard scans (right two) developed by an international group led by University of California, Berkeley researchers.
Permission granted by An (Joseph) Vu, UCSF; David Feinberg and Alex Beckett, UC Berkeley and Advanced MRI Technologies
Keeping hope alive
Experts don’t think the pinch will last forever, though. Breakthroughs in neuropsychiatry are already happening, such as the use of light and chemicals to control nerve cell activity. Imaging technologies are improving as well, offering a look at brain circuitry with never-before-seen clarity.
"If you combine imaging together with highly selective chemical tools, which are the drugs, you can begin to understand [how therapies affect] brain circuitry, and which brain regions are involved in which responses," said Hargreaves.
"This has long been a goal in the field, but I think it's become a lot better in recent years."
Bristol Myers is willing to wait, however. Rather than build a large neuropsychiatry organization around Karuna, the company is content to lean on external partners, Hargreaves said.
Other pharmas may take a similar approach. That means smaller, more specialized drugmakers will likely shoulder much of the neuropsychiatry research. Some might argue that could be for the better. Drug programs like KarXT can more easily slip through the cracks at big, multinational firms, which typically split their attention and resources across units dedicated to different diseases.
Whether the presence of these larger companies is necessary for the field to bloom is also a point of debate. Several biotechs, from Intra-Cellular Therapies to Acadia Pharmaceutical to Alkermes, have successfully developed and commercialized psychiatry drugs on their own.
What’s important, according to researchers, is to build on each incremental step and keep resources flowing into the field. “Whenever any [neuropsychiatry] news comes out, I think we have to somewhat get excited, because otherwise there would be no reason for hope,” said Gonzales. “And we have to have hope. We have to invest in the things that look promising.”
For drug developers, the brain represents a final frontier of sorts, much like ocean’s depths or the reaches of space do for other scientists. Cracking it is “not for the faint of heart,” according to Lieberman.
“At the same time, there's a huge unmet clinical need, and tremendous profitability to be had,” he said. “So that's to say, if you're up for the challenge, it's certainly worth the effort.”
Visuals Editor Shaun Lucas contributed photo research to this story.
Article top image credit: Permission granted by Bristol Myers Squibb
UniQure gene therapy slows Huntington’s progression in small study
New study data showed treatment slowed signs of disease progression by 75% after three years, a finding that could have “massive effects on patients’ lives,” an investigator said.
Though from only 12 patients who’d received the highest tested dose of the therapy, AMT-130, and had been evaluated for at least 36 months, the effects were “greater than what we even anticipated and expected and hoped for,” said Sarah Tabrizi, director of the University College London Huntington’s Disease Center, on a conference call.
Long a pioneering gene therapy company, UniQure has had multiple restarts over the years. For instance, the company developed the first gene therapy approved in Europe, Glybera, but abandoned it after poor commercial performance. UniQure then sold off rights to a hemophilia B gene therapy that’s now on the market, betting instead on a pipeline led by AMT-130.
AMT-130 is designed to silence a gene that produces a mutant form of a protein called huntingtin that damages nerve cells. Its development hasn’t been straightforward. Trial data released in 2023 suggested that AMT-130’s effects weren’t powerful enough. And while that sentiment has since changed, UniQure, like many other gene therapy makers, has been forced to cut jobs and dial back research plans to continue development.
The investment, so far, appears to be paying off. In the trial, UniQure evaluated two different dose levels of AMT-130 in 29 enrollees, and compared their disease trajectory against an external control group similar people involved in a, large longitudinal trial called Enroll-HD. The main goal was an impact on a well-known scale for evaluating the progression of Huntington’s.
The new data came from a dozen enrollees in the high-dose group who had completed enough follow-up. Those who got AMT-130 saw their scores increase by an average of 0.38 points while the controls increased by an average of 1.52, a statistically significant, 75% difference.
“That means for one year of disease progression, they will have four years longer in terms of disease-free lives,” Tabrizi said. It’s a “huge effect size, and will have massive effects on patients’ lives.”
Treatment was also associated with a 60% slowing of a second measure of progression dubbed Total Functional Capacity. This objective is “seemingly valued by FDA as it was recommended as a [Phase 3] primary endpoint” in another Huntington’s disease trial, she said.
New research kindles excitement around stem cell therapies for Parkinson’s
Two studies published in Nature found stem cell-derived products can not only be safely transplanted into the brain, but also show promising — albeit unproven — signs of efficacy.
By: Jacob Bell• Published April 16, 2025
The most effective drug for Parkinson’s disease hasn’t changed in 50 years. But fresh research published in one of the country’s top scientific journals is helping build the case for a more cutting-edge approach that uses stem cells to restore important brain functions.
The second most common neurodegenerative illness, Parkinson’s is caused by the loss of certain nerve cells. These cells produce a chemical messenger, dopamine, that plays a crucial role regulating movement. Since the 1970s, a drug called levodopa, which the body converts into dopamine, has been the mainstay treatment for combating the tremors, slowness, stiffness and balance issues that come with Parkinson’s.
Levodopa doesn’t stop the disease, however, so scientists have spent decades trying to find a more permanent fix. The latest development in that search comes from two clinical trials testing stem cell-derived therapies transplanted into the brains of Parkinson’s patients.
The first of those trials, conducted at the Kyoto University Hospital in Japan, evaluated seven people who received what are essentially blank slate cells that can turn into dopamine-producing neurons. These cells were created using a technology pioneered at Kyoto University, where roughly 20 years ago, scientists discovered how to reset some adult human cells to act like stem cells.
The study’s main focus was safety. Results, published last April in the journal Nature, show no serious adverse events were reported, though researchers did identify 73 mild to moderate events. Importantly, there was no evidence the introduced cells started growing in an unchecked, tumor-like fashion — a major concern with stem cell implants.
The study also explored whether this therapy had any effect on patients’ disease. Two years post-treatment, the six participants who were evaluable had gotten better on a scale clinicians use to measure the severity of Parkinson’s motor symptoms. Researchers looked at what’s known as “on” time, when medications are adequately controlling these symptoms, as well as the opposite “off” time, and found scores improved an average of 36% and 20%, respectively.
Another test indicated that dopamine-producing cell activity had increased substantially. This was determined through a technique in which researchers strap a radioactive element to a molecule of levodopa and then use a PET scan to follow its path through the nervous system, somewhat like how a submarine tracks objects on a sonar display.
The second trial took place at sites throughout the U.S. and Canada, and employed a different kind of stem cell that comes from human embryos. It enrolled a total of 12 participants and followed them for a year post-transplant.
Similar to the Japan study, there were no deaths, serious adverse events or tumor-like tissue growth related to the introduced cells. Trial runners did report two serious events overall. One participant was hospitalized with COVID-19, while another had a seizure that was attributed to the surgical procedure.
The trial also saw improvements in “off” scores on that disease severity scale and positive results from the radioactive levodopa test.
The cell therapy tested, called bemdaneprocel, is being developed by Bayer subsidiary BlueRock Therapeutics, which back in August 2023 announced some of the data. A Phase 3 trial began in 2025.
Hideyuki Okano, a stem-cell scientist at Keio University in Tokyo, argues more research is needed to confirm these types of cell therapies are effective against Parkinson’s.
Still, in an accompanying Nature editorial, he called the new trial results “encouraging” because they suggest treating Parkinson’s patients with donor cell transplants is likely safe. That both trials “proved to be safe, and hinted at possible efficacy, is an important step towards the establishment of this cell therapy for Parkinson’s disease in wider society,” he wrote.
Cell therapy for Parkinson’s isn’t a new idea. In 1989, a team led by neuroscientist Olle Lindvall performed the first cell transplantations for Parkinson’s patients. While the landmark study didn’t show a major therapeutic benefit, a few interesting signals encouraged the research community to keep exploring.
One ethical concern from that trial was that it used a relatively large amount of tissue derived from aborted fetuses. In the decades since, Parkinson’s and cell biology experts have made significant progress identifying other, less controversial sources of stem cells that can be scaled more easily.
A milestone of that work came in 2020, when the technique invented at Kyoto University was used to turn a Parkinson’s patient’s own skin cells into the early stages of dopamine-producing neurons, which were then implanted into his brain.
According to Okano, as of December, there were 115 clinical trials testing 83 products derived from “pluripotent” stem cells. And among those targeting central nervous system disorders, the ones for Parkinson’s disease are at a more advanced stage of development.
Further behind Bayer and BlueRock, Aspen Neuroscience, a San Diego-based biotechnology company, has a Parkinson’s therapy derived from patients’ own cells currently in early-stage human testing.
Article top image credit: Getty Images
Sodium channel blockers for pain: New opportunities after Vertex’s ‘watershed’ moment
The success of Vertex’s opioid alternative Journavx could aid a group of biotechs that aim to take a similar development path with NaV1.8 and NaV1.7 inhibitors.
By: Jacob Bell• Published July 1, 2025
In the notoriously expensive business of drug development, SiteOne Therapeutics made do with little. The biotechnology startup formed in 2010, aiming to create new, non-addictive pain relievers at a time when overdoses involving opioids were killing more than 20,000 people in the U.S. each year.
Yet the dire need for safer medications didn’t resonate with most investors. To them, pain was too risky. Scientists knew the general outline of how it worked: a cut, scald, break, pinch, slam or zap would alert special proteins and chemicals, which, like sentries, relay pain signals through the body. But the finer details of this process were — and, in many cases, still are — fuzzy, like how people who suffer the same injuries can report very different pain experiences.
This uncertainty meant SiteOne had to, for most of its life, rely on small grants to stay afloat. “There was certainly a difficult period,” CEO John Mulcahy said. “Pain was out of favor, so it was difficult to raise capital around these assets.”
That period now appears over. In the last eight months, SiteOne not only closed a $100 million fundraising round led by Novo Holdings, the controlling stakeholder of Ozempic-maker Novo Nordisk, but also agreed to sell to Eli Lilly in a deal that could be worth up to $1 billion.
The newfound interest and investment can be attributed, in good part, to Vertex Pharmaceuticals, which has led the charge investigating a group of tube-shaped, pain-regulating proteins called sodium ion channels. After a quarter century of meticulous, onerous work, Vertex’s labs finally crafted a channel-blocking molecule the company viewed as safe, effective and precise enough to help address the opioid epidemic.
In January 2025, the Food and Drug Administration approved this molecule, known commercially as Journavx, as a treatment for the sharp, short-lived “acute” pain felt after an accident or surgery. Ken Harrison, a senior partner at Novo Holdings, said a core reason his firm decided to back SiteOne was that Vertex had established these drugs can be successfully studied and brought to market.
While Journavx has so far proven remarkably safe and absent of addictive properties, doctors remain torn about how useful it will ultimately be for patients. At its best, the drug looks to be only as potent as a weak opioid. At least 5,800 Journavx prescriptions were written during the third week of June; millions more will need to come for it to meet Wall Street’s blockbuster forecasts.
Still, TD Cowen analysts recently described the drug’s approval as a “watershed moment that could pave the way for a new era of non-opioid pain treatments.” Indeed, SiteOne and at least 10 other developers want to follow in Vertex’s footsteps with their own medicines that stopper either the “NaV1.8” sodium ion channel, as Journavx does, or a close cousin, “NaV1.7.”
A person holds two pills of Vertex Pharmaceuticals’ new drug for moderate-to-severe pain, Journavx.
Permission granted by Vertex Pharmaceuticals
What are sodium channel inhibitors, and how do they work?
Found in the outermost layers of many cells, these proteins function like faucets for charged sodium particles. They open in response to various stimuli — a bright light switching on, a bite of a salty food, a handful of ice from the freezer — at which point ions flood into the cell. This rush creates an electrical pulse that travels through the nervous system and to the brain, where it's used as information to determine how the body should feel and react.
Of the nine known types of sodium ion channels, three are primarily found in the peripheral nervous system, where they play key roles in pain signaling. The signaling process resembles a line of dominoes. At the start is the root of the pain, at the end the brain. By blocking these channels, scientists are effectively removing a couple of the earliest tiles so they can’t continue the cascade.
“You’re stopping the pain as close as you can to the source,” and leaving “other modalities of sensory signaling intact,” explained Stephen Waxman, a neurology professor at the Yale School of Medicine who’s made significant discoveries about the role ion channels play in pain, on a 2023 podcast run by The New England Journal of Medicine.
For drugmakers, NaV1.7 and NaV1.8 have emerged as the two most popular pain targets. One reason is their location; being on the outer edge of the nervous system, rather than thoroughly embedded in organs like the heart or brain, reduces the risk that channel-blocking drugs will disrupt other vital body functions.
These proteins also work in different ways, offering researchers a shot at treating a variety of pain types. NaV1.7 acts like a light switch, abruptly turning the pain signal on and off, while NaV1.8 is more akin to a dimmer. SiteOne’s Mulcahy has said NaV1.8 could therefore be a more desirable target for chronic pain management, since the goal there usually is not to shut pain off, but to dial it back down to “normal.”
Designing medicines that bind to a specific sodium channel remains exceptionally challenging, as the subtypes all share very similar structures. Additionally, the proteins move extremely fast — opening and closing in milliseconds — and are exposed to relatively large electrical fields. Only in the last 15 or so years, with the creation of new tools, have drugmakers been able to adequately study and precisely drug ion channels.
What are the advantages over other drugs for pain?
Scientists believe that, by avoiding the central nervous system, sodium channel blockers can alleviate pain without eliciting the side effects or addictive risks posed by opioids. The late-stage studies that led to Journavx’s approval support this theory.
Together, the two trials recruited more than 2,000 people who had just undergone either a “tummy tuck” surgery or a bunion removal. Participants received either Vertex’s drug, a placebo, or a combination of Tylenol and a commonly prescribed opioid that served as an “active comparator.” Investigators found lower rates of nausea, dizziness and headache among those given Journavx than in the other groups.
Journavx was generally safe and well-tolerated, according to Vertex, and nearly all of the adverse events seen in these studies were mild to moderate in severity. Drug-treated patients did, however, show higher rates of itchiness, rash and muscle spasms compared to their placebo-treated counterparts.
As for its effectiveness, Journavx proved significantly better than the placebo at alleviating acute pain. Both trials measured this with a 0-to-10 scale wherein patients rate their pain intensity at a series of time intervals over two days.
Notably, the drug was not more effective than the active comparator regimen. That’s raised debate about its ultimate utility in a setting like acute pain, where both patients and healthcare providers are typically looking for a powerful, quick-acting medication. While Vertex leadership has maintained this finding won’t deter doctors from prescribing Journavx, some pain experts have described the pill’s effects as modest. Richard Vaglienti, medical director of the Center for Integrative Pain Management at West Virginia University, even classified the results as “glaring.”
That could leave the door open for other developers to compete — even those working outside the field of sodium ion channels. In May, Pittsburgh-based Viatris reported positive results from late-stage studies evaluating a reformulated version of an old medication, an “NSAID” called meloxicam, in people who had bunion removal or hernia repair surgeries. Viatris said its drug didn’t just beat a placebo at providing acute pain relief, an after-the-fact analysis found it also offered “significantly superior pain control” to tramadol, an opioid less potent than the one used in Vertex’s studies.
Following this release, Brian Skorney, an analyst at the investment firm Baird, noted how Viatris’ data “highlight a number of concerns we have with Journavx’s profile, in particular, onset of action, a critical factor for post-operative pain.”
The results, Skorney argued, make Journavx “look like an inferior option” compared to a “pretty old” drug. “If NSAID’s don’t have the highest efficacy, as Vertex is fond of saying, what does that say about Journavx?” he wrote.
Which companies are developing NaV1.7 and NaV1.8 inhibitors?
The majority of developers researching sodium ion channels for pain are small biotechs.
One, Dogwood Therapeutics, formed in 2024 through the reverse merger of Wex Pharmaceuticals and Virios Therapeutics. It had 12 full-time employees at the end of December. Another, Channel Therapeutics, had four, and is now in the process of combining with a subsidiary of drug commercialization specialist Ligand Pharmaceuticals.
Such deals could suggest that, while this area is receiving more attention, building a company around it remains challenging and may require less conventional methods for raising money at a time when investors are viewing biotech more skeptically.
Other players include Praxis Precision Medicines, Newron Pharmaceuticals, RaQualia Pharma and Xenon Pharmaceuticals. Two more, Sangamo Therapeutics and privately held Navega Therapeutics, are taking a genetic approach, with therapies built to suppress the gene that encodes for NaV1.7 proteins.
Latigo Biotherapeutics is further ahead, and like SiteOne touts a drug aimed at NaV1.8 in mid-stage testing. That drug, LTG001, is being evaluated in acute pain following a tummy tuck, bunionectomy or wisdom teeth removal.
Latigo is backed by prominent life sciences investors such as Westlake Village BioPartners, 5AM Ventures and Alexandria Venture Investments, and last March announced the closing of a $150 million funding round that CEO Nima Farzan said should keep the company going at least until it has late-stage data for LTG001.
Vertex and Eli Lilly, with its pending purchase of SiteOne, currently appear to be the sole big pharmaceutical firms in this space, though others have shown interest. AbbVie had “ABBV-318,” an oral molecule designed to inhibit both NaV1.7 and NaV1.8, but no longer lists the drug in its pipeline. Scientific American reported last year how Merck & Co.’s patent activity also suggests it may be stealthily exploring ion channels for pain.
A Merck spokesperson said the company is “committed to neuroscience research,” including chronic and acute pain. “At this time, it’s too early to share information related to sodium ion channel inhibitors, but we will continue to collaborate with scientists and investigators worldwide to advance innovation and find solutions that may address complex and debilitating neurological diseases.”
At Vertex, company leaders are trying to expand Journavx’s approval beyond acute pain and into chronic, though testing has thus far delivered mixed results.
Article top image credit: K_E_N via Getty Images
Bristol Myers’ prized schizophrenia drug stumbles in testing
A late-stage study found Cobenfy wasn’t better than a placebo as an add-on to atypical antipsychotics. Some analysts view the failure as a “significant hit” to the drug’s commercial outlook.
By: Jacob Bell• Published April 23, 2025
A brain drug at the center of a recent $14 billion acquisition has failed a large clinical trial, leading some Wall Street analysts to substantially lower their sales forecasts.
Bristol Myers Squibb closed a deal to acquire the drug, Cobenfy, and its developer in March of 2024, about six months before it was approved in the U.S. as a schizophrenia therapy. While launching Cobenfy, Bristol Myers has simultaneously been working to get the drug cleared for other uses, such as adding it on top of atypical antipsychotics for the treatment of schizophrenia.
But that work has now hit a setback. In April 2025, Bristol Myers disclosed that an almost 400-person study found its drug not significantly better than a placebo in this setting.
All participants in the study were given atypical antipsychotics, with about half taking Cobenfy and the other half a placebo. Using a well-known, 210-point scale that measures the severity of schizophrenia symptoms, researchers found scores in the Cobenfy group improved by 14.3 points. Though that change was roughly two points better than the placebo arm, it wasn’t enough to hit the trial’s main goal.
Bristol Myers said it will further analyze the results and discuss them with regulators and the medical community. The company also plans to present more detailed data at a medical conference.
"When patients are already receiving treatment, demonstrating additional statistical benefit becomes inherently more difficult,” said Husseini Manji, a professor in Oxford University’s psychiatry department and co-chair of the U.K. government’s Mental Health Goals program, in a statement from Bristol Myers.
“Although Cobenfy did not demonstrate a statistically significant improvement as an adjunctive treatment in this trial, the data are encouraging,” Manji added. “These findings warrant additional follow up and may provide valuable direction in our ongoing search for complementary approaches to address these persistent treatment gaps.”
Analysts view Cobenfy as a vital revenue driver for Bristol Myers, which soon stands to lose patent protection on two of its most lucrative products — the blood thinner Eliquis and the cancer immunotherapy Opdivo. Yet the trial failure has some rethinking Cobenfy’s commercial outlook. David Risinger, an analyst at Leerink Partners, previously predicted that Cobenfy revenue would reach $5.8 billion in 2030. But he cut that forecast to $2.6 billion.
In a note to clients, Risinger claimed the failure indicates Cobenfy is only modestly effective, igniting fears among his team that the drug has “far less potential than we originally anticipated.”
Sean McCutcheon, from the investment bank Raymond James, lowered his 2030 estimates, too, from a little over $3.7 billion to a little under $3 billion. He also removed the adjuvant schizophrenia opportunity from his model.
According to McCutcheon, perhaps the biggest consequence of the study failure is that it might increase the perceived risk of Cobenfy succeeding in the “myriad” other conditions in which it’s being tested. Those include bipolar disorder, autism spectrum disorder and symptoms associated with Alzheimer's disease like agitation and psychosis.
Others, though, don’t appear as worried. William Blair analyst Matt Phipps still sees a “significant commercial opportunity” for the drug in schizophrenia and, potentially, Alzheimer’s psychosis. And Carter Gould, of Cantor Fitzgerald, argues the trial’s outcome isn’t as dire as it might seem. Bristol Myers said there were underlying trends favoring Cobenfy, for example.
In his own client note, Gould highlighted how not only was Cobenfy already being used as an adjuvant schizophrenia treatment ahead of the trial results, but feedback given to the Cantor team from some influential doctors suggested they would keep prescribing the drug even if it missed in this setting.
“Bigger picture, the optics around a negative top-line result for one of the bright spots in the commercial portfolio aren’t great, but there’s likely enough here on efficacy for psychiatrists to justify continued and growing use of the drug in schizophrenia,” Gould wrote.
Article top image credit: Permission granted by Bristol Myers Squibb
ALS drugs from Denali, Calico come up short, marking setback for Healey trial
Denali’s medicine and a similar one from Calico Life Sciences and AbbVie were not much different than a placebo, results that reinforce the difficulty of ALS drug research.
By: Jacob Bell• Published Jan. 7, 2025
A landmark study hoping to find new treatments for ALS has notched two more failures, as experimental medicines from Denali Therapeutics and Calico Life Sciences proved no better than a placebo at slowing the nerve-destroying disease or keeping patients alive longer.
Denali disclosed high-level results in early 2025. After about six months, treatment with the company’s drug didn’t result in any significant changes in the severity of the disease, nor did it substantially help patients’ muscle strength or respiratory function.
Denali plans to further examine the data and look at biological markers of the disease, including one, “neurofilament light chain,” that’s become increasingly important to researchers focused on amyotrophic lateral sclerosis.
“Though the initial top-line clinical results of this trial were not what we hoped, the data collected is valuable in helping to understand the next stage of ALS research,” said Merit Cudkowicz, director of the Sean M. Healey & AMG Center for ALS at Massachusetts General Hospital, in a statement.
Cudkowicz and her team came up with — and for years have been running — the “Healey platform trial,” an innovative experiment structured to quickly test a variety of potential ALS therapies. The trial has so far evaluated more than half a dozen drugs, but none have successfully hit its main goals.
Alongside the Denali news, the Healey center announced a similar medicine from Calico and AbbVie had failed, too. Both Denali’s and Calico’s drugs are supposed to activate “eIF2B,” a complex molecule cells use to make proteins. Research indicates stress and disease inhibits this molecule, which in turn can exacerbate the accumulation of stress-related proteins like TDP-43.
While helpful when functioning normally, TDP-43 can, under certain conditions, become a bad actor in nerve cells. It is tied to ALS and other neurodegenerative diseases, and has therefore attracted interest from a handful of brain-focused biotechnology companies. In late 2024, a San Francisco-area startup launched with a drug designed to work around this TDP-43 problem. Named Trace Neuroscience, the startup came equipped with $101 million from a group of prominent life sciences investors that includes Third Rock Ventures, Atlas Venture, RA Capital Management and Alphabet’s venture capital arm, GV.
Cudkowicz said the Healey team remains “deeply committed to fully understanding the effects” of Denali’s drug and will “further evaluate the data before determining next steps.”
Some Denali investors may not be willing to wait, however. Shares of the company fell more than 6% following news of the trial setback. Calico is a privately held subsidiary of Google parent Alphabet.
“This was always a low expectations, high-risk study” for Denali, wrote Michael Yee, an analyst at the investment bank Jefferies, in a note to clients. The failure of AbbVie and Calico’s therapy to also hit the same goals in its own study arm points to “a difficulty with the drug class in a challenging disease.”
In its own statement, Calico pointed to an assessment of muscle strength that hinted at slower deterioration among those given the company’s drug. Bill Cho, the company’s head of clinical sciences, said the finding “supports further investigation.”
Like many brain diseases, ALS has been exceptionally difficult to crack for even the world’s most powerful drug developers. Only a few medicines have received approval from the Food and Drug Administration, and their effects are considered modest. Patients still typically live just two to five years following a diagnosis.
The list of approved therapies got shorter after Amylyx Pharmaceuticals voluntarily removed its once-promising medication Relyvrio from the market. Amylyx made that decision once a key study meant to confirm the Relyvrio was an effective ALS treatment instead found it no better than a placebo.
Article top image credit: Getty Images
New postpartum depression drugs are here. Diagnosis, treatment hurdles still stand in the way.
Two Sage Therapeutics medicines are approved for the condition. But uptake of the first has been minimal, while the launch of the second is still getting off the ground.
By: Delilah Alvarado• Published April 10, 2024
Editor’s note: This story was published in April 2024. Sage Therapeutics has since been acquired by Supernus Pharmaceuticals in a deal completed July 31, 2025.
When Katherine Wisner began studying postpartum mental health in the 1980s, the field barely existed. Relatively little research was focused on psychiatric illness related to pregnancy, and postpartum depression wasn’t yet well understood.
Wisner, now an associate chief of perinatal mental health at Children’s National Hospital in Washington, D.C., recalls a senior male supervisor dismissing a case she flagged of a new mother experiencing severe depression and suicidal thoughts. “You have to be wrong,” she remembers him responding. “Women aren't depressed in pregnancy, because they're fulfilled.”
For years, the idea that having a baby is one of the happiest times in a mother’s life persisted despite research indicating that’s not always the case. Over time, though, researchers and physicians began to acknowledge the range of mental health effects a postpartum woman can experience, spurring research into medicines that might help.
Now, doctors in the U.S. have two drugs they can prescribe specifically for postpartum depression, or PPD, a condition that affects an estimated 1 in 8 women following birth and can be severe. Both are from biotechnology company Sage Therapeutics. An intravenous injection called Zulresso was approved in 2019, while a daily oral pill called Zurzuvae got clearance in 2023.
Their approvals were many years in the making. Yet both come with risks and limitations, and adoption has been slow — a fact some experts attribute to still-evolving awareness of PPD, and how to treat it.
“We are not recognizing it as a country and as a society,” Wisner said.
Slow recognition
Mental health professionals have relied on a guidebook called the Diagnostic and Statistical Manual of Mental Disorders, or DSM, to diagnose and treat their patients for more than 70 years.
But the DSM didn’t recognize PPD until the 1990s, when its fourth edition codified the condition as a “major depressive disorder occurring within four weeks of giving birth.”
The next edition, in 2013, went a bit further, defining PPD as a major depressive episode occurring during pregnancy or within four weeks after giving birth. The most recent update also highlights possible coexisting symptoms of anxiety and panic.
“Slowly the field grew so that eventually there actually was a formal diagnosis of depression,” said Wisner.
The drawn-out recognition of PPD left women dealing with the condition to fend for themselves for decades. It wasn’t until 2015, for instance, that the American College of Obstetricians and Gynecologists issued its first guidance on screening for symptoms in both pregnant and postpartum women.
“Historically, the messaging was that pregnancy is the greatest time in a woman's life, and there's no happier time than after a baby’s delivered,” said Julia Riddle, a reproductive psychiatrist and assistant professor at the University of North Carolina School of Medicine. “And it took a lot to really demonstrate that, maybe, it's a little more complicated.”
Difficulties in diagnosis
Even with formal screening recommendations, diagnosis can still be challenging. Questionnaires like the Edinburgh Postnatal Depression Scale and the Patient Health Questionnaire are often used by doctors to determine whether new mothers may be experiencing PPD or anxiety.
If PPD is suspected, psychotherapy, or “talk therapy,” is typically the first option. Drug intervention is usually reserved for more severe cases or for women who were previously on medication.
Actually receiving treatment can be a hurdle, too. Michelle Visser, a mother and psychotherapist for pregnant and postpartum women, recalled how few people asked about her mental health after she gave birth.
“A lot of people don't necessarily know when they need help, because people aren't talking about it,” Visser said. “You don't know what you don't know.”
Partly as a result, PPD is often underdiagnosed and, even when it is, not well treated. According to the Centers for Disease Control and Prevention, approximately 60% of women with symptoms of postpartum depression go undiagnosed, and half of those diagnosed aren’t treated.
“People tend to do the [Edinburgh] scale and then move on,” said Judith Joseph, a psychiatrist at NYU Langone Health and a researcher on trials of Sage’s PPD drugs. “Many times, there's shame in reporting any type of sadness to the provider because if your baby's happy and healthy, you should be happy and healthy too.”
Moreover, not every OB-GYN is trained to treat PPD since it has not always been a part of standard care. Access to therapies can also vary depending on a person’s insurance coverage, resources, or other health concerns.
These medicines can help, but their effects don’t usually kick in for four to 10 weeks, if at all. The evidence supporting their use in PPD is also limited.
“When people are having depression, that impacts their functioning and their quality of life,” Joseph said. “Telling them they'll get relief in eight to 10 weeks is very difficult to hear for someone who has a lot of responsibilities, who wants to be able to bond with their child, who wants to be able to get back to the life that they once had.”
Antidepressants can also cause weight gain, gastrointestinal issues, agitation and sleep disturbance.
Doctors need to evaluate prospective patients for bipolar disorder before they prescribe an antidepressant, too. Up to 1 in 5 people screened for PPD may instead have bipolar disorder, a mental illness that causes mood swings and psychosis. Antidepressants can exacerbate bipolar disorder.
Additionally, treatment can be a difficult choice for pregnant or postpartum women, who may feel pressured to go without therapy or fear a drug might affect their child through breastfeeding. (Breastfeeding while on medication doesn’t necessarily present a risk to the infant, however.)
“There is stigma because people assume that motherhood should be inherent to being a woman,” Joseph said. “But [people] don't necessarily acknowledge the challenges.”
Socioeconomic status, ethnicity and familialsupport can also affect how someone might view receiving help.
“We treat in the medical system, for the most part, people of color totally different,” Visser said. “Those families are very concerned they're going to be seen as unfit parents and that action will be taken against them.”
A sparse drug pipeline
Despite a push for better treatments, the development of drugs specifically for PPD has been sluggish. Research has largely centered on psychotherapy and existing antidepressants.
“We weren't even recognizing these [postpartum] illnesses decades ago, so we weren't going to do trials trying to find a medication specifically for these illnesses,” said Nancy Byatt, a perinatal psychiatrist and professor at UMass Chan Medical School.
Compounding the difficulty is the fact that clinical studies have historically not always included women, nor have drugmakers focused on illnesses that primarily affect women. Clinical trials frequently exclude pregnant women over concerns an experimental drug may harm a fetus and, as a result, researchers don’t know as much about how different types of drugs can affect pregnant women.
Enrolling postpartum women in trials is complicated, too, as the window of time to test a therapy is small.
“It’s still hard because we're talking about nine months. People are often not talking about their pregnancy until three months in,” Riddle said. “So you have a very brief time to consent them, get them onto a protocol and follow them into the postpartum. It's a hard thing to study.”
A box of Sage Therapeutics’ postpartum depression drug Zurzuvae
Permission granted by Sage Therapeutics
Sage has been one of the few biotechnology firms to try. The company set out early last decade to develop the drug that became Zulresso, which was approved in 2019 for moderate-to-severe PPD. Its modest efficacy and 60-hour infusion requirement has kept adoption minimal, however.
Working with Biogen, Sage later developed an oral drug called Zurzuvae that it sought to get approved for both PPD and in major depressive disorder. In 2023, the FDA approved it for PPD, but not MDD — a blow to the company that led to layoffs.
Earlier academic research had set the stage for Sage’s drugs. Studies found that depressive symptoms caused by changes in certain brain chemicals during pregnancy might be alleviated with drugs that act onso-called GABA-A receptors. Both of Sage’s PPD drugs are synthetic versions of a neurosteroid called allopregnanolone, a brain hormone that affects GABA-A receptors. They essentially work similarly to hormone therapy, suggesting the role hormones might play in PPD.
“For a long time, it's been debated whether postpartum depression is just another form of major depressive disorder or it's an entity by itself,” said Bassem Maximos, an OB-GYN in League City, Texas and a trial investigator. “A lot of us OB-GYNs believe there has to be a different mechanism because a lot of our patients are different from regular major depressive disorder patients.”
Beyond Sage’s drugs, the pipeline of therapies in development for postpartum depression is thin. Brii Biosciences, another biotechnology company, has a drug in mid-stage testing, but there are few others.
Will PPD drugs succeed?
While Zulresso and Zurzuvae’s approvals were a milestone for PPD drug research, neither has been widely used.
Zulresso’s lengthy administration must take place in a healthcare facility, keeping adoption low, while Sage faced pushback for the drug’s $34,000-per-course price tag. Sales were $6.7 million in Zulresso’s first full year on the U.S. market, and only $10.5 million in 2023.
The FDA, as well as psychiatrists like Byatt, agreed Zulresso’s “benefits outweigh the negatives.” But the drug’s requirements make it a hard sell, especially for women who lack additional support, or are a single parent.
Zurzuvae, which launched commercially in the U.S. in December 2023, is more attractive. As an oral medicine, the drug can be shipped to a patient’s home and is taken daily for two weeks. Still, sales have been been only modest at best.
Zurzuvae takes effect rapidly, which could help it stand out compared to other medications, such as SSRIs, that have a slower onset of action. In clinical trials, Sage also found its drug could relieve symptoms of anxiety.
“The fact that this medication works quickly, and also gives [patients] that added relief for sleep and anxiety is beneficial compared to an SSRI that works slower, and may not necessarily relieve sleep and anxiety as rapidly,” Joseph said.
While Zulresso’s and Zurzuvae’s side effects are modest, both carry black box safety warnings. Zulresso’s warns of excessive sedation and loss of consciousness, while Zuruvae’s cautions of impaired ability to drive. However, Maximos claims the drowsiness was a “positive side effect” for some mothers in the clinical trials who suffered from a lack of sleep and exhaustion.
“It's exciting that we're here,” Riddle said “It's exciting that women have spoken up about their struggles, and that women have taken the time to say, ‘hold on, [motherhood] was actually hard.”
Beyond drug-specific challenges, new mothers face other hurdles that can impact PPD care. Paid maternity leave is not guaranteed in the U.S. and many women are in so-called maternity care deserts, making finding adequate support difficult.
“We always want better treatments that work but the reality is we're not getting the treatments we have to the people who need it right now,” Wisner said. “That's where the big gains are going to come from.”
In an effort to make treatment easier, Sage and Biogen have launched a patient support program, and are working with organizations on PPD education initiatives.
Some experts think a bigger change around culture and access is needed, however.
“The main way that we could possibly address mental health — what's been a crisis for years and is now an emergency — is by supporting resilient and healthy families, and we have to start with perinatal mental health to be able to do that,” Byatt said.
Still, there is some optimism. Joseph sees Sage’s approvals as opening the door to more drug research, for instance.
“This is an opportunity to pave the way for a huge amount of research in this space,” Joseph said. “It's just the beginning.”
Article top image credit: Getty Images
The future of neuroscience drug development
Despite several pullbacks in the field in the last decade, there are signs neurology is again a priority in some corners of the industry. Biotech companies have drawn big-name backers as they’ve moved promising brain drugs into late-stage testing, and new medicines for Alzheimer’s, ALS and depression show a path to market.
included in this trendline
UniQure gene therapy slows Huntington’s progression in small study
In AbbVie deal, Wall Street sees momentum for psychedelics M&A
Sodium channel blockers for pain: New opportunities after Vertex’s ‘watershed’ moment
Our Trendlines go deep on the biggest trends. These special reports, produced by our team of award-winning journalists, help business leaders understand how their industries are changing.